

Journal of the Bahrain Medical Society
Year 2018, Volume 30, Issue 2, Pages 31-37
https://doi.org/10.26715/jbms.2_12b082018Moutasem Almashour1*, Hazem Al-Aali1, Eslam Mohamed2
1Consultant, Anesthesia and Pain Management, Salmaniya Medical Complex, Ministry of Health, Kingdom of Bahrain.
2Anesthesia Resident, Salmaniya Medical Complex, Ministry of Health, Kingdom of Bahrain.
*Corresponding author:
Moutasem Almashour, Consultant, Anesthesia and Pain Management, Salmaniya Medical Complex, Ministry of Health, Kingdom of Bahrain; Tel: (+973) 17284288, Email: moutasem73@hotmail.com
Received date: April 08, 2018; Accepted date: August 12, 2018; Published date: September 21, 2018

Background and objectives: Cancellation of cases on the day of surgery carries significant burden on the patient’s health and the facility. The study aimed to evaluate the rate and causes of cancellation of surgeries.
Methods: In this observational study, 46,496 operations were studied between the years 2016 and 2017. The records of the main operation theater were examined at the Salmaniya Medical Complex to evaluate the rate and causes of cancellation of operations. Cancellation was defined as a surgery that was not performed after the patient entered the operation theater on the day of surgery.
Results: The prevalence of cancellation was 0.92%. The main cause for cancellation was high blood pressure (41.2%), followed by cardiac issues (7.3%) and upper respiratory tract infections (6.8%). Further, 3.7% of the cancelled surgery cases were due to lengthy list. While grouping the cancelled surgeries based on specialization, it was observed that the highest (28.9%) cancellation rate was in the general surgery. Poor utilization of the preoperative assessment clinic was observed in 9.3% cases in the main operation theater during the year 2017.
Conclusion: Despite the low cancellation rate in Salmaniya Medical Complex, as compared to other centers, improvement in the preoperative care and assessment would further reduce the cancellation rate significantly.
Keywords: Cancellation, Salmaniya Medical Complex, preoperative care, surgery, operation theatre
Cancellation of a surgical procedure on the day of the surgery carries a significant burden on the patient’s health and the health facility, which results in poor utilization of the theater time and resources.1, 2, 3 It also increases the cost and waiting time for elective surgeries. In elective cases, cancellation rate varies between centers and despite improvements in medical and administrative services, many surgical cases are cancelled in the operative room due to causes that can be avoided/ optimized.4, 5, 6
The aim of this study is to review the causes and rate of cancellation of surgeries (the operation not performed at the specified time) in the operation theater. Further, classification of these causes into broad categories and to provide recommendations that would reduce the cancellation rate.
In this retrospective, observational study, the causes of cancellation of surgeries in the operation theater at Salmanyia Medical Complex were evaluated between January 2016 and December 2017. After obtaining the approval of the hospital health research (ethical) committee, the data were collected from the register of the cases that got cancelled in the main operation theater before administering anesthesia.
It is worth noting that the office of the main operation theater records all the cases cancelled in the main operation theater, day-case unit theater, burn unit theater, endoscopy unit, and the labor room. Salmaniya Medical Complex is the main tertiary care referral hospital in the Kingdom of Bahrain, with 21 operation theatres performing approximately 25,000 cases per year. It is the only hospital in Bahrain performing renal transplants and advanced neurosurgical procedures. The main operation theater of Salmaniya Medical Complex deals with both elective and emergency surgeries.
In this study, cancellation is defined as a surgery case that was cancelled after the surgery was scheduled and the patient was taken into the operation theater. The theatre staff (nurses) document the main reason of cancellation in the register of the operation theatre. This is done after the surgical and anesthesia consultants fill a specific cancellation form covering the theater, which includes the patient’s biodata, type of surgery, and the specific reasons for cancelling the surgery. Data was collected for all patients, including inpatient and day case (same day surgery), elective or emergency surgeries. The manual collection of data included the number of scheduled cases, number of cancellations, the reasons, and the surgical specialty.
The cases that were scheduled and the patient didn’t attend, cases scheduled for local anesthesia, cancellation from the ward, and cancellations from operation theaters where the cancellation forms were not submitted such as in Jidhafs maternity, hospital radiology suite, psychiatry hospital, bone marrow biopsy cases, and pediatric oncology cases were excluded from the study despite a sizable number of cases (1617 in 2016 and 1803 in 2017). The overall cancellation rate was calculated from the total number of cancellations divided by the total number of the booked cases.
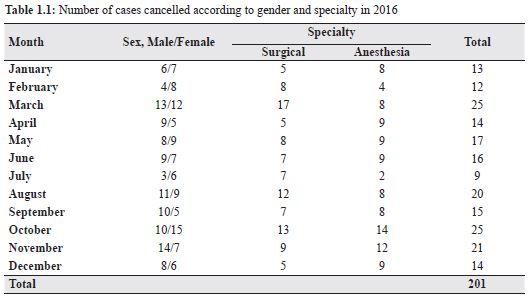
A total of 46,496 cases (23,320 in 2016; 23,176 in 2017) were registered to enter the operation theater, of which, 429 cases (0.92%) were cancelled. Cases cancelled during 2016 and 2017 summed up to 201 and 228 cases, respectively with cancellation rates of 0.86% (2016) and 0.98% (2017). Among the cancelled cases during the two years, 247 (57.5%) males and 182 (42.42%) females were reported (Tables 1.1 and 1.2). Causes of cancellation were categorized in the official cancellation form as due to anesthesia or surgical cause.
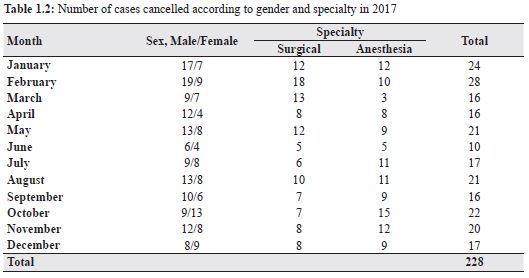
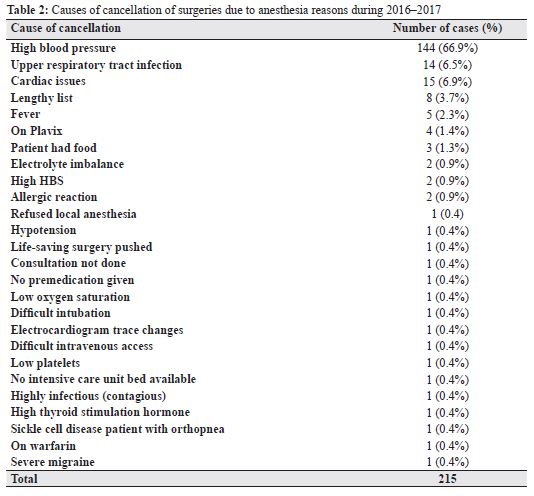 The total number of cases cancelled due to the cause of anesthesia (Table 2) in the 24 months comprised of 215 (50.1%) cases. The highest number of cases were cancelled in the month of October 2016 and 2017, respectively. Whereas, the lowest number of cancelled cases was during February and March 2017; noticeable reasons are due to uncontrolled high blood pressure followed by cardiac issues and upper respiratory tract infections. It is worth mentioning that 3.7% of the cancellations were due to lengthy list assigned that could not cope with the theater allocated time.
The total number of cases cancelled due to the cause of anesthesia (Table 2) in the 24 months comprised of 215 (50.1%) cases. The highest number of cases were cancelled in the month of October 2016 and 2017, respectively. Whereas, the lowest number of cancelled cases was during February and March 2017; noticeable reasons are due to uncontrolled high blood pressure followed by cardiac issues and upper respiratory tract infections. It is worth mentioning that 3.7% of the cancellations were due to lengthy list assigned that could not cope with the theater allocated time.
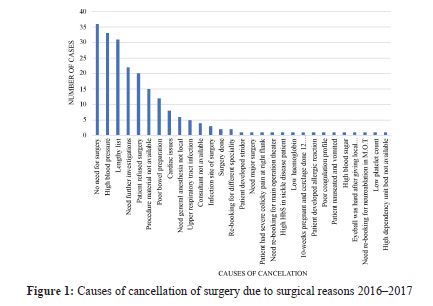
Due to the surgical causes, 214 cases were cancelled, which comprise 49.8% of the total cancelled surgeries as indicated in Tables 1.1 and 1.2. Highest and lowest number of cancelled cases due to surgical reasons were observed during February and June 2017. In 2016, highest and lowest number of cancelled cases were seen in the month of March and January. The most common reasons for cancellation were no requirement of surgery (33; 15.4%), high blood pressure (33; 15.4%), and lengthy list of cases (31; 14.4%; Figure 1).
When further classifying the cancellations based on surgical specialization, it was noted that the highest (62; 28.9%) rate of cancellation was observed in general surgery, followed by endoscopy (38; 17.7%) and (29; 13.5%) ophthalmology units, respectively (Table 3).
Cancellation of a planned surgical case on the day of the surgery carries a significant burden on the patient’s health from many perspectives and on the facility, such as poor utilization the theater time,1, 3 improper utilization of the resources, and increased cost and waiting time for elective surgeries.2, 7, 8
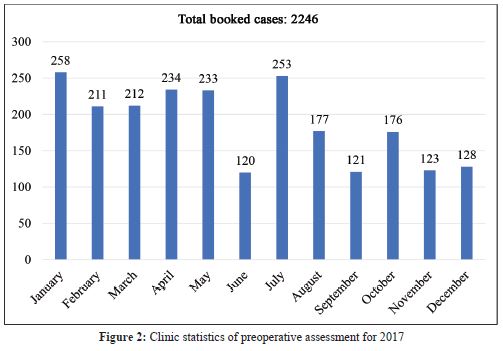
The cancellation rate of elective cases differs from one hospital to other; some hospitals reported cancellation rate < 10%,4, 5 while other centers defined a rate as high as 24%.6, 9 Lacqua et al. reviewed 1063 cases and reported a cancellation rate of 17%.10 Similarly, Chang et al. reported 0.21% cancellation rate after patients entered the operating room.11 Whereas, our study revealed overall cancellation rate for two consecutive years (2016 and 2017) at Salmanyia Medical Complex to be 0.92%. Despite improvement of the medical and administrative services, many surgical cases are cancelled in the operative room due to causes that can be avoided/ optimized beforehand. Studies12, 13 indicate that preoperative evaluation and preparation of patients both in the ward and the preoperative clinic before scheduled surgeries have many benefits. One of the many benefits include proper optimization of the patient’s medical conditions leading to a reduction in cancellations of cases on the day of surgery.14, 15 The preoperative assessment of the patients done in the preoperative clinic is 9.3% of a total number of cases done in the main operation theater in 2017 according to the medical records statistics (Figure 2) which is low compared to the total number of patients operated on. Despite that, the cancellation rate in Salmanyia medical complex is low compared to other centers.
Further, evaluating the cases, which were cancelled, they can be categorized as “avoidable” and “unavoidable” causes.16, 17 Avoidable causes, such as cases cancelled due to high blood pressure (41.2%) of the total cancelled cases during the years 2016 and 2017, can be optimized.
It is worth noting that cancellation of these cases was justified by their operation team as they carry high risk to the patient’s life that supersedes the benefits in relation to the type of surgery. Amongst the cancelled cases, labeling these cases as “temporarily unfit for surgery” and bringing them later for surgery after being optimized, carries extra burden on the facility that could have been avoided if adequate care was given to the patient earlier.
On the other hand, cancellation due to unavoidable reasons, which include acute change in the patients’ medical status (acute upper respiratory tract infection),16, 17 anaphylactic reaction, and theater being occupied due to lifesaving procedures were minimal in the list of causes.
Cancellation or postponing the surgery from the economical side carries great burden on the facility and patient himself from loss of working days and the hospital cost. According to the Agency for Research and Quality,18 hospitalizations that include a surgical procedure account for nearly half of all hospital costs. Thus, ensuring optimal use of theater time by reducing the period of hospitalization, and delay of surgery will reduce the hospital expenditure.
The cancellation rate in Salmaniya Medical Complex is low compared to other centers. There is room for improving the care of the patients entering the operation theater, and thus, reducing cancellation rates of the scheduled surgeries. Optimization of patients in the perioperative clinic and proper allocation of time in case of lengthy lists of surgeries, communication with the operation theater staff with regard to availability of equipment, and evaluation of laboratory reports of the patient prior to transferring the patient to operation theater can further reduce the cancelation rates of the surgical cases.
We hope, from this study, to highlight the significance of the cancelation of cases in the operating room and the importance of reducing the rate. Further, improvement in the recording method in the main operation theater, such as electronic format should be implemented for accurate and easier access to the information. Future studies are required to validate the improvements.
To date, this is a first study to include a large volume of cases (46,496) in the Salmaniya Medical Complex with regard to surgical services in the Kingdom of Bahrain. Nonetheless, there were several limitations to this study, including retrospective, single-facility study, and the information was obtained manually from the main theater records. The record had limited data and was poorly organized for the proper differentiation of the main cause of cancellation i.e. anesthesia, surgical, facility, and patient cause.
We acknowledge the ethical committee and operation theater of the Salmaniya Medical Complex and Dr. Wafa Al-Mansoori, Directorate of Vocational Reviews.
The authors of the study have no conflict of interest to declare.