
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2019, Volume 31, Issue 1, Pages 5-9
https://doi.org/10.26715/jbms.2019.1_26022019aHytham Ghanem1*, Mohammad Tanvir Khan2, Salah Al-Ghanem3, Ghada Al-Qasem4
1Senior Resident, Pediatric Emergency Department, Bahrain Defense Force Hospital, Royal Medical Services Hospital, Kingdom of Bahrain.
2Senior Resident, Emergency Department, Bahrain Defense Force Hospital, Royal Medical Services Hospital, Kingdom of Bahrain.
3Consultant Emergency Medicine, Emergency Department, Bahrain Defense Force Hospital, Royal Medical Services Hospital, Kingdom of Bahrain.
4Consultant Pediatric Emergency and Head of Emergency Department, Bahrain Defense Force Hospital, Royal Medical Services Hospital, Kingdom of Bahrain.
*Corresponding Author:
Hytham Ghanem, Emergency Department, Bahrain Defense Force Hospital, Royal Medical Services Hospital, Kingdom of Bahrain; Tel: 17766477, Email: hma765@yahoo.com
Received date: January 07, 2019; Accepted date: February 26, 2019; Published date: March 31, 2019

Fishing, swimming, diving, and other water-based recreational activities are popular in the Kingdom of Bahrain and the Arabian Gulf. In this case report we describe a case of stonefish poisoning encountered by a 44-year-old fisherman on the coasts of Bahrain. Human envenomation is rare, and the Arabian Gulf is not the usual habitat of the stonefish. No accurate data is available on the incidence or international frequency of stonefish envenomation. This article describes the treatment and difficulties encountered with his management. We also review the proper management, medical guidelines, and care of stonefish poisoning. The patient presented with severe excruciating pain and edema of his upper limb. He was administered with intravenous analgesia for pain control and was admitted under surgical care for further management of impending compartment syndrome and underwent a fasciotomy. An antivenom for stonefish may be used, however is not available in Bahrain. He was discharged following treatment after 5 days of hospitalization. Although, stonefish is rare in our region, stonefish sightings have been reported in the Arabian Gulf. Management of stonefish and marine envenomation involves soaking the affected site in warm water to denature the venom, analgesia, and stonefish antivenom.
Keywords: Fish envenomation, fish poisoning, stonefish, Syneceiea verrucosa
The Kingdom of Bahrain is an archipelago of 40 islands located off the coast of Saudi Arabia in the Arabian Gulf. For more than 2000 years, Bahrain’s pearls have been prized as the best natural pearls in the world and a large part of Bahrain’s economy relied on Pearl fishing—the diamonds of the sea—as one of the most valuable resources.1 Even the French jeweler Jacques Cartier made many journeys to Bahrain from 1810 until 1923 to buy pearls until it became victim to cheap competition in the 1930’s.1 Bahrain is well known for fishing and the waters of the Gulf are inhabited by over 200 species of fish, such as sea urchins, sting rays, jelly fish, fire fish, and the well-camouflaged stonefish.2, 3
Venomous fish are a threat to swimmers and divers all over the world. The family Scorpaenidae represents a large variety of fish with the ability to envenomate with their spines. These include the lionfish, scorpion fish, bull trout, and the stonefish, which is known as the most venomous fish in the sea. Human envenomation is a rare presentation in the Arabian Gulf, since it is not the usual habitat of the stonefish. There are around 100 reported medical cases of stonefish envenomation, however they are uncommon in the region of Bahrain.4, 5 It is usually found in the northern coasts of Australia, coastal waters of Indonesia, India, Singapore, China, Philippines, and Japan, and Caribbean sea waters and the Red sea.6, 7
We are unaware of any medical case reports of stonefish envenomation in Bahrain or the Arabian Gulf;8, 9 however, stonefish species have been reported in the coasts of the Arabian Gulf.3, 10
 Figure 1: Stonefish
Figure 1: Stonefish
The stonefish is usually brown or grey, and it may have areas of yellow, orange, or red. It usually lies motionless and partially buried in the sand to camouflage within corals and rocks. The most common form of injury is when it is stepped on or kicked, and less commonly by touching or handling the fish. It has 13 dorsal spines that can penetrate a shoe with a soft sole. Each spine contains around 5–10 mg of venom, which is released from the spine upon contact as a defensive mechanism.11
The clinical features of human envenomation include the presence of puncture wound sites and severe local pain. The puncture site is inflamed and sometimes cyanotic; the surrounding area is hypersensitive, pale, and swollen with tender swollen surrounding lymph nodes. It may commonly be associated with nausea, vomiting, sweating, fever, cardiogenic shock, respiratory distress, and possible death in severe cases, which is very rare.8, 9
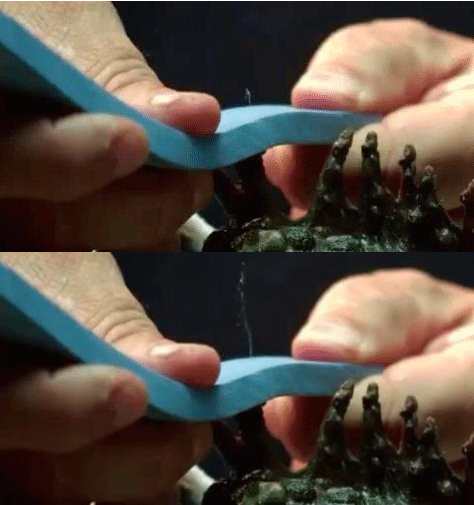
Figure 2: Venom is released from glands on the base of spines when pressure is applied
Seqirus CSL is an effective antivenom for stonefish stings, which was developed at the Common Wealth Serum Laboratories (Melbourne, Australia).4 It is made by immunizing horses against the stonefish venom then collecting the part of the horse’s blood, which neutralizes the poison. The antivenom is purified and supplied in a vial consisting of 2000 units of stonefish antivenom, sodium chloride, phenol, and substances of horse blood.5
A 44-year-old fisherman, originally from India, presented to the Emergency Department (ED) at the Bahrain Defense Force Hospital. The victim was brought to the ED by his colleagues after being stung by a reef fish. The patient reported seeing a brown fish that looked like a rock or coral on the sea bed with a spine on its back, which he initially thought was a rock and touched it with his index finger. He reported rapid onset gross edema and severe pain radiating up his right arm and was initially taken to a local health center near the fishing site. Analgesics were administered and was advised to seek medical care at our Hospital’s ED. The fisherman was brought to the ED six hours after the incident.
On initial assessment there was an obvious puncture wound on the palmar aspect of his right index finger with no active bleeding or discharge from the wound site (sting site) with gross swelling of his whole hand, including the wrist and distal forearm. The patient described severe pain ascending up to his forearm and numbness of his hand. Initial vital signs showed a pulse, blood pressure, and temperature at 70 beats/ min, 188/99 mmHg, and 36.4°C, respectively. On examination, he was oriented, alert, and was in severe pain; airway, breathing, and circulation were intact.
The patient’s right radial pulse was palpable and was equal on both hands with good peripheral circulation and normal peripheral capillary refill time; sensation was intact. He was able to move his hand and fingers, although it was severely painful. Based on the patient’s history, his description of the fish, and following his confirmation of the fish by showing him photos, a diagnosis of stonefish envenomation was made (ICD T.63.5 Toxic effect of contact with fish).
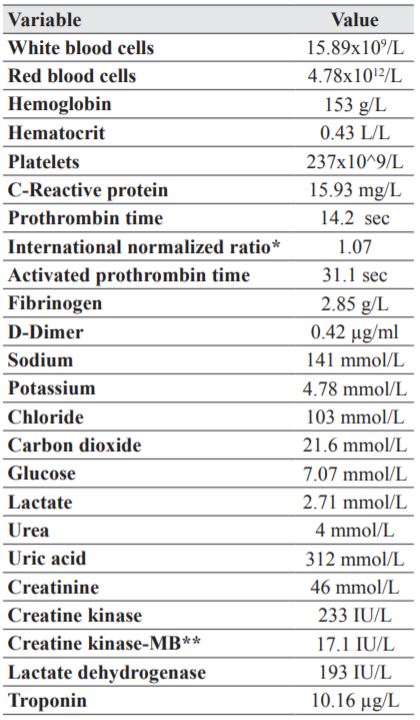
Routine biochemical tests were performed (Table 1). Analgesics [Intravenous (IV) Fentanyl 100 mcg and Perfalgan 1 gm IV] were administered to relieve the pain and intravenous fluids were initiated. We attempted to find an antivenom for stonefish venom, however there was no antivenom available in our hospital as well as in the Kingdom of Bahrain.
Table 1. Results of routine blood test
After the pain was controlled using analgesics, the patient was admitted to the inpatient wards for further care. Following admission, the patient underwent fasciotomy of his right forearm under general anesthesia for impending compartment syndrome of his right hand (compartments were released, hemostasis was secured, and dressing was applied over wounds). He was started on Cefuroxime 500mg oral tablets 12 hourly for 1 week and was kept on diclofenac sodium 100 mg oral tablets 24 hourly for 5 days for pain control. During hospital stay, he underwent daily wound dressing after which the swelling reduced gradually; patient was discharged after 5 days of hospital stay. There was no record of his follow-up after discharge.
Although, toxic spine fish injury is very rare in the region of Bahrain, stonefish sightings have been reported in the Arabian Gulf as well as Bahrain. Considering the unavailability of the antivenom in the Gulf, we present this case report describing our encounter and also as a review of the management of such cases.
This is a unique presentation since stonefish or even marine envenomation is very rare in our region, and we are not aware of any medically reported cases in this region. Our patient presented with a typical history and symptoms of stonefish envenomation (excruciating pain and severe swelling of his affected limb). In view of these envenomations, management guidelines need to be reviewed in order to properly manage such patients, especially awareness to warm water soaking, which may have been beneficial to denature the protein. Also, immediate pain relief should have been started with our case prior to presentation at our hospital.4,5 Antivenom is also available for severe cases, however it is not available in our region.
Generally, the prognosis is good with full recovery.5, 8 Patients may develop complications related to marine envenomation that are associated with significant morbidity, especially hand envenomation, and can result in joint contractures, compartment syndrome, necrotic ulcers, and infections. Severe complications that lead to death are usually associated with anaphylactic reactions to the venom.4, 8
Fishermen and divers should be aware of these fish and their appearances and should wear protective puncture proof gloves or shoes. Swimmers or waders at beaches should not do so barefoot, especially during the night or in poor visible conditions. It is also important to mention that stonefish may be still venomous for up to 48 hours after their death. It is important not to touch or handle marine animals unnecessarily since the most effective tactic is avoidance.4, 5, 8
The venom produced is a heat-labile toxin, which is a high molecular weight protein and is made up of four main biological fractions: (1) Hyaluronidase fraction, (2) capillary-permeability factor (3) toxic/ lethal fraction, and (4) pain production factor. It has a pH of 6.0, and can be denatured by heat, acid, or alkali (pH>9.0 and pH<4.0). It’s heat labile property is the basis of treatment.4 The capillary permeability factor contributes to the severe edema and may also be responsible for extensive pulmonary edema. The toxic fraction (Stonustoxin SNTX) is a potent hypotensive agent with neuro/myotoxic effects.4, 12 Stonefish antivenom is available and produced from Common Wealth Serum Laboratories (Melbourne, Australia). It is used for patients with significant pain or systemic symptoms. The antivenom is administered intramuscularly at a dose of 200 units (1 ampoule) for every 1–2 puncture wounds to a maximum of 3 ampoules.4
The most important immediate action/treatment is to immerse the affected hand or foot in hot water. This is the “Gold standard” for treatment of all marine envenomation and should be initiated immediately even prior to arrival at hospital as this will help denature the heat-labile protein,4, 11 and usually brings almost immediate relief of pain in most patients. The recommended temperature of immersion is 45°C (or as hot as the patient can tolerate) for at least 30 min and up to 90 min or until removal of the limb from water no longer results in recurrence of pain.5, 9, 13 For further pain control, nonsteroidal antiinflamatory drugs (NSAIDs) or opioids can be administered. The wound may be infiltrated with local anesthetics without epinephrine, if pain relief is still required.
In severe cases, stonefish antivenom may be used, which is administered intravenously or intramuscularly and is capable of neutralizing venom of Indo-Pacific and Atlantic stonefish species.4, 5, 9, 13 Infected puncture wounds should be cultured in selective media for Vibrio species. Wounds should be cleaned and inspected for foreign bodies (specifically for spines); radiographs or ultrasounds may be helpful. Blisters often contain active venom and result in dermal necrosis if not excised.12
All marine wounds are at a risk of developing secondary infections. Antibiotics are important in the management and are recommended. Antibiotic prophylaxis should be targeting the following bacteria for all marine injuries and envenomation: Vibrio, Aeromonas, Mycobacterium marinum, and Erysipelothrix rhusiopathiae. 12 Patients should also receive Tetanus prophylaxis.4, 11, 12
Many injuries may be mistaken for envenomation and the differential diagnosis for marine injuries is large. Species commonly inhabiting certain coasts may aid in the differential diagnosis along with the mechanism and description of injury. Differentials of stepping on sharp objects may include stonefish poisoning, sea urchins or sharp corals, or debris. Detailed history and description of the injuring fish or even photo confirmations are important to confirm the diagnosis.15, 16
Management of stonefish and marine envenomation involve immediate soaking of the affected site in warm water to denature the protein in the venom and should be done prior to presenting to the hospital. This will also provide immediate pain relief. Analgesics are used for pain control. In severe cases, a stonefish antivenom may be administered, if available. All marine wounds are at risk of secondary infection and prophylactic antibiotics are important in the management.
The authors of this study have no conflicts of interest to declare.