

Journal of the Bahrain Medical Society
Year 2014, Volume 25, Issue 1, Pages 5-8
https://doi.org/10.26715/jbms.p25_2Adel Salman Al-Sayyad,*, ** Randah R. Hamadeh*
*Department of Family and Community Medicine, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Kingdom of Bahrain.
**Disease Control Section, Public Health Directorate, Ministry of Health, Manama, Kingdom of Bahrain.
Correspondence to: randah@agu.edu.bh

Background: The negative effects of climate change on human health and well-being are widely documented in recent literature. The poorest countries, and the most vulnerable and marginalized individuals, experience the worst consequences from climate change. Laborers are more prone to climate-related conditions (CRC) as they are considered one of the under-privileged populations with low salaries and unfortunate living and working conditions.
Objectives: To measure the burden of CRC on health services in the main laborers’ clinic in the Kingdom of Bahrain.
Methods: A cross-sectional study of expatriate workers who attended Al-Razi Health Centre (ARHC) during the study period. A convenience sample was selected and a specific questionnaire was designed for the purpose of this study. The variables included in the questionnaire were age, gender, nationality, occupation, work setting, diagnosis including CRC, medications prescribed and length of sick leave given. CRC were identified and grouped by a panel of experts in line with the published literature.
Results: Out of a total number of 3,715 visits during the study period, CRC visits represented 1,111 with a proportion of 29.9%. The majority (70%) of the CRC patients were working solely outdoors. Infectious diseases were the most common (62.9%) CRC followed by heat-related diseases (16.5%).
Conclusion: CRC have a significant burden on the health services at ARHC. CRC appear not to be significantly associated with age, nationality or place of work of laborers.
Keywords: climate; weather; laborers; outdoor jobs; Bahrain
The negative effects of climate change on human health and well-being are widely documented in recent literature.1-3 An increase in mortality related to thermal extremes and weather disasters and a higher incidence of food- and waterborne-related infections and other climate-related conditions (CRC) have been reported.4-5 Climate change can affect the basic requirements needed to support and sustain human health such as good quality food, clean water and air, and shelter.5, 6 CRC include several groups of conditions, e.g. vector-borne diseases7 and heat-related mortality,8, 9 malnutrition,1 allergies,10 infectious5, 7 and diarrheal diseases.8
Although climate change is a global phenomenon, the poorest countries and the most vulnerable and marginalized individuals in all countries will experience the worst consequences from it.2, 11 The most vulnerable groups to the disease burden resulting from climate change include elderly people, patients with pre-existing medical conditions, children, and the poor, especially women, traditional societies, subsistence farmers, and outdoor workers.5, 6, 13
Laborers are more prone to CRC as they are considered one of the underprivileged population with low salaries and unfortunate living conditions.5, 6 Climate changes have several direct effects on laborers and working people such as heat exhaustion and heat stroke,12 in addition to the indirect effects such as increased risks for infectious diseases and vector-borne diseases, malnutrition, water and sanitation problems, injuries due to extreme weather events, and stress and mental health issues.5, 13
In 2010, the population of Bahrain was 1,234,571 of whom 568,399 were Bahraini and 666,172 non-Bahraini. Primary health care in Bahrain is delivered through 24 health centres distributed all over the country with Al-Razi Health Centre (ARHC) being the only centre assigned for workers and the main one for pre-employment screening. The services at ARHC include pre-employment examination and primary care for expatriate workers and company employees.14 Although the majority of the expatriate workers receive treatment at ARHC, they may receive health services from other health centres, company clinics, and private hospitals and clinics. In 2010, 249,577 expatriate workers, representing around 37.5% of the total non-Bahraini population were registered at ARHC.15 The majority of patients attending ARHC are Asians mostly from India, Pakistan, Sri Lanka, Bangladesh, Philippines, Indonesia, and Nepal.
The aim of this study was to measure the burden of CRC on health services in the main laborers’ clinic in the Kingdom of Bahrain.
This was a cross-sectional study of expatriate workers who attended ARHC during the period 1st to 14th August 2008. ARHC received 168,979 visits with an average of 463 visits per day during that year.14 A convenience sample of all attendees during the study period was selected and a specific questionnaire was designed for the purpose of this study. The variables included in the questionnaire were age, gender, nationality, occupation, work setting, diagnosis including CRC, medications prescribed and length of sick leave given. CRC were identified and grouped by a panel of experts in line with the published literature.1
Expatriate workers who were diagnosed by the attending physicians and identified by the researchers to have CRC during the study period were interviewed. Data collection took place during the morning and evening shifts of the health centre. Data entry and analysis were performed using SPSS version 12. The burden of CRC was measured by calculating the proportion of CRC visits to the total number of visits during the study period, number of drugs prescribed for CRC patients and number of lost working days. The Chi Square test was used to evaluate significant differences.
Out of a total number of 3,715 visits during the study period, CRC visits accounted for 1,111 with a proportion of 29.9%. The age of the laborers ranged from 18 to 62 years with most of them in the age group 26-35 years (48.1%). More than three quarters of the patients were Indians (76.2%), and a similar proportion (74.1%) were morning shift workers with the majority (70%) working solely outdoors (Table 1). Figure 1 shows CRC types among the laborers by each condition and Figure 2 when the conditions were grouped. Infectious diseases were the most common (62.9%) followed by heat-related diseases (16.5%). The number of prescribed drugs for CRC patients was 2,604 with 88.5% of the patients receiving at least 2 medications (Table 2). A total of 1,515 days of sick leave were issued for CRC patients with 35.0% of these patients given two days sick leave or more (Table 2). Statistically significant associations were observed between CRC and length of sick leave, and number of drugs prescribed (Table 3).
Table 1. Demographic characteristic of laborers presented with climate-related conditions at Al-Razi Health Centre, Bahrain
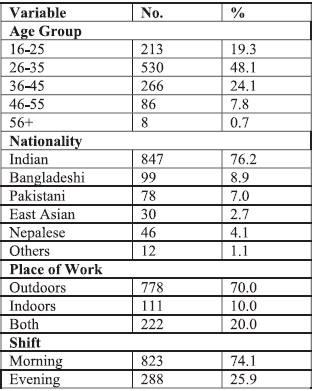 Table 2. No. of drugs and sick leave length prescribed to laborers presented with climate-related conditions at Al-Razi Health Centre, Bahrain
Table 2. No. of drugs and sick leave length prescribed to laborers presented with climate-related conditions at Al-Razi Health Centre, Bahrain
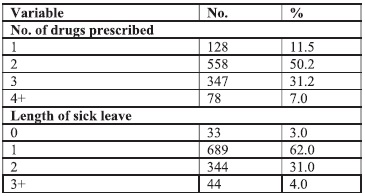
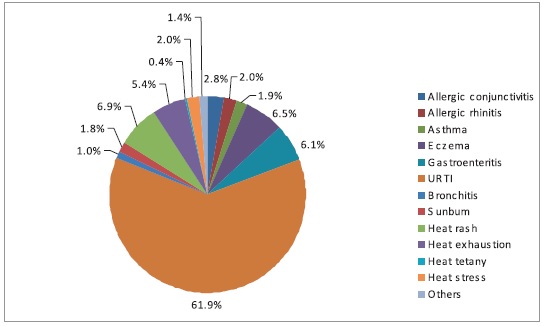 Figure 1. Distribution of CRC among patients who attended Al-Razi Health Centre, August 2008
Figure 1. Distribution of CRC among patients who attended Al-Razi Health Centre, August 2008
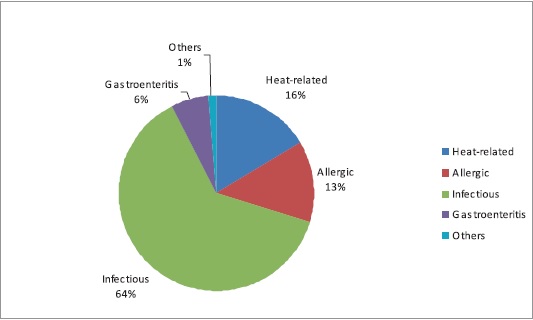
Figure 2. Types of CRC among patients who attended Al-Razi Health Centre, August 2008
Table 3. Demographic characteristics and climate related conditions among laborers at Al-Razi Health Centre, Bahrain
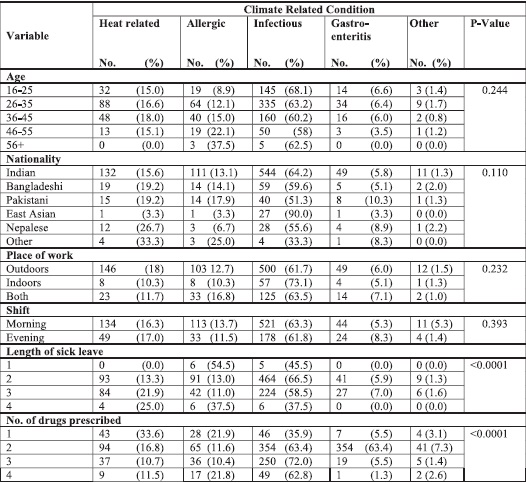
Most of the patients were young and the majority of these were Indian nationals. This simply reflects the age distribution and nationality of expatriate workers in Bahrain who are young and come mostly from India.14 Most of the laborers occupied manual unskilled outdoor jobs such as construction work. This made them more prone to develop heat-related conditions as they produce more intra-body heat caused by their physical labor.15 It also explained the high percentage of heat-related conditions which ranked second only to upper respiratory tract infections among them. This is in accordance with a previous study reporting that the mean average number of admissions to the emergency department at the Salmanyia Medical Complex (SMC) was 4.6 patients per day when the mean average heat index was 69.1° C, and declining to 2.4 patients per day when the heat index decreased to 54° C. This study also noted that the majority of the patients were non-Bahraini (97.4%) with laborers in the age group 23 to 41 years, mostly coming from the Indian subcontinent.16 These findings were not dissimilar to those reported in other Gulf countries.17
The economic cost of the CRC is high as illustrated by the high absence rate that reduces the work force and affects the economic welfare of the country. In addition, the high prescription rate for CRC, increases the direct costs to the health system by reallocating additional financial resources on medications. The increase of CRC cost for both the laborers and health services is well documented in the literature.18
In conclusion, although CRC have a significant burden on ARHC health services they do not appear to be significantly associated with age, nationality or place of work of laborers.
This study is based on the project of the Assessment of the Vulnerability of Human Health to Climate Change in the Kingdom of Bahrain Report. In: The Second National Communication under the United Nations Framework Convention on Climate Change, 2012. Special thanks go to the medical students of the College of Medicine and Medical Sciences, Arabian Gulf University for data collection.