
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2014, Volume 25, Issue 1, Pages 19-23
https://doi.org/10.26715/jbms.p25_5Jaleela S. Jawad,* Adel Salman AlSayyad,* Kubra S. Nasser*
*Public Health Directorate, Ministry of Health, Manama, Bahrain
Correspondence to: aassayyad2000@yahoo.com

Background: In 1996 Bahrain and other members of the Gulf Cooperation Council (GCC) formulated a tuberculosis elimination initiative. The objective of this initiative was to decrease the incidence of smear-positive pulmonary tuberculosis to 1 per 100,000 by 2010.
Objective: To describe the trend of tuberculosis incidence rates and the characteristics of tuberculosis cases in Bahrain.
Methods: A retrospective descriptive study of surveillance data of all TB cases diagnosed in Bahrain between January 2000 and December 2006, collected from Salmaniya Medical Complex, Ministry of Health, and medical records. Additional sources were accessed for tuberculosis records. Data were entered, validated and analyzed using SPSS-16 statistical package. Frequencies and cross tabulations were generated. Categorical variables were tested using the Chi Square test.
Results: Over the seven-year study period, 1,584 tuberculosis cases were diagnosed in Bahrain. There was a slight rise in the overall incidence of tuberculosis among both Bahrainis and non-Bahrainis with little or no downward trend; however, this remained low among Bahrainis, ranging from 12.5 to 16.8 per 100,000 per year. The incidence was higher among non-Bahrainis ranging from 47.4 to 75 per 100,000. Asians were the commonest non-Bahraini nationality with tuberculosis. The incidence of pulmonary tuberculosis was higher than extra-pulmonary tuberculosis in both Bahrainis and non-Bahrainis with male predominance in both groups. Among Bahrainis, the most affected were those over 65 years of age.
Conclusion: Despite the rising incidence of TB in Bahrain, migrant workers were the major contributors to this increase. TB incidence among Bahrainis was low.
Keywords: tuberculosis; incidence; rate; surveillance; TB; expatriate workers
Tuberculosis (TB) is one of the major causes of mortality in the world. It is an infection caused by mycobacterium tuberculosis and is predominantly transmitted by aerosol from sputum-positive patients who usually have a cavitating disease. The lungs are generally affected causing pulmonary TB (PTB); however, other sites may be involved causing extra-pulmonary TB (EPTB). The spread of infection in a community is facilitated by a number of factors with overcrowding perceived to be one of the major ones. Additional factors include poor living conditions and inadequate ventilation and illumination. Prisons and shelters are also common sites where infection may be readily transmitted.1, 2, 3
Despite the efforts undertaken to control TB, the global burden remains enormous. According to a WHO global report, the incident cases estimated in 2010 were 8.8 million (8.5-9.2). TB-related deaths were estimated at about 1.2 to 1.5 million, and of these 1.1 million were in people who were HIV negative and approximately 0.35 million more among those who were HIV positive. India and China had the highest rank of notified cases in 2010 followed by Africa accounting, collectively for about 24% of notified cases.4
There are few studies describing TB in the Gulf Cooperation Council (GCC) states. However, the impact of a high influx of expatriate workers coming from TB endemic countries is on the rise and, accordingly, the incidence in GCC states has been addressed frequently within these few studies.5,6 Moreover, the trend in TB notification rates was examined in a study conducted in Oman showing a decline in the rate of TB notification among Omanis, with males aged more than 50 years representing the main group.7 On the other
hand, recently an upward trend in the TB incidence was observed in all GCC member states apart from Oman which reported TB among Omanis only.5 A study conducted in Saudi Arabia describing the TB epidemiology found that the highest incidence rates were among the elderly, while children were the least affected.8
The incidence of tuberculosis in Bahrain was examined in a previous epidemiological study for the years 1965, 1971, 1980-1981 and 1983-1987.9 A sharp decline was observed in the incidence and mortality rate since 1965. Non-Bahrainiss howed rates which were on average about seven times higher than Bahrainis. In 1987, the age distribution of cases among Bahrainis shifted to older age groups in comparison to previous years, and in all the study years there were more males with pulmonary tuberculosis than females. Most TB
cases notified were among non-Bahrainis, the majority being single adult male Asian workers. 9, 10
According to a policy which was implemented in 1982, all non-Bahraini TB cases were to be repatriated after receiving initial TB treatment. TB is a notifiable disease in Bahrain and cases of pulmonary TB should be notified within 24 hours of diagnosis while EPTB should be notified within a week of the diagnosis.10 All data of reported cases is centrally recorded, registered and archived at the Public Health Directorate while the treatment registry is kept centrally at Salmaniya Medical Complex (SMC). Bahrain is considered to be one of the countries with a low-tointermediate prevalence according to the global report year 2011.4
The aim of this study is to describe the demographic and clinical characteristics of TB cases in Bahrain and to determine the trend of TB incidence in Bahrain over the study period.
A retrospective observational descriptive study of TB cases across the study period (from 2000 to 2006) was carried out from central registry at the Public Health Directorate and Salmaniya Medical Complex, which is the main government hospital where all TB cases in Bahrain are registered and receive TB treatment.
All diagnosed TB cases (Bahraini and expatriates) during the specified period of the study were included in the study (1,584 cases). Cases were identified as having TB by positive sputum smear examinations, culture, histology, radiology and/or were based on clinical diagnosis. Patients initially diagnosed as having TB and started on therapy but later found to have another disease were excluded from the study.
A data collection sheet was designed and used to collect data about age, sex, nationality, occupation, marital status, smoking status, and type of TB, site of TB and year of diagnosis. Data were collected from the patients’ records at SMC, the TB registry in the TB ward in SMC, hospital admission and discharge records, Public Health Laboratory records, TB electronic records and public health diseases notification records.
Data were entered and analyzed using SPSS-16. Simple descriptive statistical analysis was computed for demographic and clinical variables.
The denominator used for calculation of TB incidence by nationality and age category is the Central Informatics Organization (CIO) estimation of the Bahrain population projected from the year 2001 census.11 This was used for calculating the year 2001 to 2006 incidence rates. For the year 2000, the denominator was estimated based on the year 1991 census.12 The term “incidence rate” used for the purpose of this study indicates the total number of TB cases diagnosed in a year per 100,000 population.
Table 1. Demographic characteristics of tuberculosis in Bahrain, 2000-2006

The cases were classified as either pulmonary TB (PTB) or extra-pulmonary TB (EPTB) based on the WHO definitions. This classification helped in the calculation of TB incidence by type. The EPTB was further classified as to its subtype (lymphadenitis, abdominal, genitourinary, meningeal, miliary and others). This information was extracted from the medical records. If the total number of cases was fewer than 5 in any TB subtype during the 7-year period they were considered in the ‘others’ category.
Data were anonymized by assigning a unique study number to each case, and the corresponding study number and identifier were kept in a separate record (Compact Disc). Approval of the study was received from the Ministry of Health technical research committee.
A total of 1,584 TB cases were diagnosed and registered for treatment in Bahrain during the study period. Bahrainis accounted for 446 cases (28.2%) and the remaining 1,138 were non-Bahrainis. The overall mean age was 36 years with a median age of 33 years (SD 14.69). For non-Bahrainis the mean age was 33 years (median 31); however, the mean and median was higher for Bahrainis with values of 43.7 and 43.2 years, respectively. Over the study period the male-to-female gender ratio among all TB cases was 1.8:1. For non-Bahrainis, males represented almost double the number of females (2:1); however, the male-to-female ratio among Bahrainis was 1.2:1. More than half of the cases were unmarried (58.1%) with 38.5% married, widowed (2%) and divorced cases (1.3%). Furthermore, most non-Bahraini cases were from Asian TB-endemic countries. More than half (53.7%) of the patients were smokers.
PTB represented the majority of TB cases (61.8%), followed by TB lymphadenitis (24%) as the highest among the EPTB. Among PTB cases, Bahrainis were 24% (235) and 76% (744) were non-Bahrainis. The distribution of cases in each subtype is demonstrated in (Figure 1).

Figure 1. Distribution of TB cases by subtypes
Overall, there is an increasing trend in the TB incidence rate in Bahrain in the period 2000-2006. There was a slight decrease in the overall TB incidence for the period from 2000 (33.3/100,000) to 2002 (29.0/100,000). This was followed by a rise in the overall incidence rates starting from 2003 (37.2/100,000) until 2005 (38.0/100,000) with a slight decrease in 2006 (37.0/100,000). The test for the trend in the overall TB incidence rate in relation to the years of the study was significant with a P value of 0.023.
In 2000, the PTB incidence rate was 25.5 (95% CI 21.7, 29.9) per 100,000 population and by the end of year 2006 it had decreased slightly to 23 (95% CI 19.8, 26.8) per 100,000 population. These figures show that there is no real decline in the PTB incidence rate.
The EPTB incidence rate in 2000 was 7.9 per 100,000 population, rising in subsequent years - twofold by 2003 (16.9 per 100,000 population) over the baseline incidence rate. By 2006 the incidence rate had declined to 14 per 100,000 population (Figure 2).

Figure 2. Total incidence of TB by type in Bahrain (2000-2006)
The overall incidence rate among Bahrainis shows an increasing trend over the years with slight fluctuations. In 2000, the incidence was 12.5 and it rose to 16.8 per 100,000 population per year by end of 2006.
PTB incidence for Bahrainis shows a decreasing trend over time. It was 9.9 per 100,000 population in 2000; however, the incidence for 2001 jumped to 14.8 per 100,000 population, indicating an increase in the overall incidence from year 2000 to 2001. This was followed by a drop in the total incidence for 2002; then an upward trend in the overall incidence was observed for 2003 and 2004. For the following years until 2006, the rate was observed to be hovering around 7. In 2006 it was reported to be 7.6 per 100,000 population. However, the incidence for EPTB continued to increase up from 2.5 per 100,000 population in 2000, peaking in 2004 and reached 11.9 per 100,000 population per year. Then, it dropped back to 9.2 in 2006; however, the EPTB incidence has remained higher than PTB over the last two years (Figure 3).

Figure 3. Incidence of TB by type among Bahrainis (2000-2006)
The trend for non-Bahrainis was similar to the overall TB incidence trends in the Kingdom with increased incidence of both PTB and EPTB; however, compared to the overall TB incidence trends, non-Bahrainis had a higher incidence in each (Figure 4). The peak in PTB incidence was seen in 2000 (49.1/100,000); while for EPTB the highest incidence was observed in 2003 (32.8/100,000). PTB incidences were higher than EPTB incidence throughout the seven years of the study. Furthermore, the incidence of PTB among non-Bahrainis was higher than Bahrainis across the study period. The incidence among non-Bahrainis fluctuated from 2.5 to 5.2 times higher than the TB incidence among Bahrainis (Figure 4).

Figure 4. Incidence of TB by type with 95% CI among non-Bahrainis
Among Bahrainis, the proportion of TB cases distributed throughout the years was lowest among the age categories 0-4 and 5-14. The most affected age category was ≥65 years. At the beginning of the study the proportion of TB cases among aged ≥65 years was 59 per 100,000 population per year. It rose to 73.5 per 100,000 population in 2001. Then, it peaked in 2002 reaching 110.3 per 100,000 population. This was followed by a decline in 2003 and 2004. Furthermore, there were increases in 2005 and 2006 with proportions of 83.6 and 87.5 per 100,000 population per year, respectively. The total number of Bahrainis with PTB aged ≥65 years was 67 out of 234 patients (Figure 5).

Figure 5. Total TB incidence by age categories among Bahrainis
TB incidence in non-Bahrainis was inconsistent. It occurred across most of the age categories during the seven years; however, similar to Bahrainis, those below the age of 14 years were the least affected age group (Figure 6).
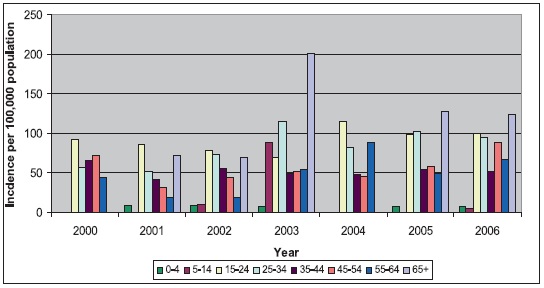
Figure 6. Total TB incidence by age categories among non-Bahrainis
The results of this study were consistent with the findings of studies conducted in the other Gulf states.5, 7, 13
Age distribution was skewed for non-Bahrainis by migrant labour status, tending to be of working age and predominantly male. Therefore, the gender ratio would be different from that of Bahrainis. The overall gender ratio among TB cases in the study showed males to be almost double that of females. This finding of a greater number of males among TB cases was supported by other studies.14, 15 The occurrence of TB more frequently in males compared to females is more likely explained in the social context rather than by genetic factors. This, however, is still debatable.16, 17
Among Bahrainis, those aged over 65 years had higher TB incidence rates compared to younger age groups. This finding was consistent with the finding of a previous study that studied TB in Bahrain.9 This could be explained by the improvement in the standard of living and health for those in the younger age group. In contrast, the elderly are at increased risk of reactivation. The overall incidence rates of TB in Bahrain increased from 33.3 to 37 per 100,000 population. This increase occurred in both Bahainis and non-Bahrainis. The finding of upward rising trends of TB were supported by the finding of another study conducted in Kuwait.5 Furthermore, this rise in the incidence rates could be a genuine increase in the number of cases or improvement in case detection and diagnosis (ascertainment bias). On the other hand this increased incidence could be further explained by the change in the population structure, especially that the denominators used for calculation were estimated numbers from previous censuses.
The trends in the incidence rates for Bahrainis and non-Bahrainis varied. For Bahrainis, PTB incidence rates were decreasing while EPTB among them is increasing across the study period. This finding interestingly differed from what was found previously in Bahrain where the overall incidence among Bahrainis was declining and EPTB incidence was not rising.9 It was also observed that the overall incidence rates among migrant workers was higher than for Bahrainis.9 The lower rates among Bahrainis could be explained by TB under-diagnosis or due to less disease incidence among them. On the other hand, the higher rates among non-nationals could be attributed to the higher prevalence of TB in the country of origin with contributions from a range of socio-economic factors.9, 13 These non-Bahraini workers are usually males who travel alone to Bahrain as their visas do not allow family entry. This further explains the higher frequency of TB in males as they are likely to live in shared accommodation which provide increased opportunity for new infections. For TB incidence rates calculations the denominator (total population at risk during that period) was a projection from previous censuses resulting in uncertainty around the denominator and may over or under represent the TB estimations.
Despite the overall increase of the TB incidence rates in the Kingdom, Bahrain still is considered to be a low prevalence country. Adult males were the predominant population and a shift to older age groups is recognized. Moreover, the dominant TB type was PTB. The majority of TB cases in Bahrain were among expatriates from TB endemic countries. Non-Bahrainis had higher TB incidence rates compared to Bahrainis. Moreover, due to the increased EPTB among Bahrainis, it is important to consider the possibility of EPTB among elderly Bahrainis with fever, weight loss and non-specific symptoms.
We support the Global STOP TB efforts as it is a great challenge to develop and implement strategies for TB control among workers coming from high burden countries. We are also advocates of mycobacterium fingerprinting in order to accurately evaluate the TB incidence and the impact of migrants on TB incidence in Bahrain.