
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2014, Volume 25, Issue 1, Pages 29-32
https://doi.org/10.26715/jbms.p25_7Manal Al-Alawi,* Nadia Sarhan,*
*Primary Health Care Section, Ministry of Health, Manama, Kingdom of Bahrain
Correspondence to: Malawi2@health.gov.bh

Background: Anemia in children is a frequent problem. Worldwide, it affects 25% of the population ranging from 64.6% in Africa to 3.4% in North America. Iron deficiency is the main cause of anemia. Even though studies indicate that the percentage of anemia among preschool children is decreasing in Bahrain, it is still considered high and needs immediate intervention.
Objective: To estimate the prevalence of anemia among nine-month-old infants attending child screening services in local health centers during the month of July 2012, and to examine the correlation between hemoglobinopathies and anemia in mothers during pregnancy and anemia in infants.
Methods: This was a descriptive, retrospective study. The records of 1,378 nine-month-old infants attending mother and child care for child screening services in all local health centers during July 2012 were studied.
Results: 1,230 infants (89.3%) had hemoglobin level test done. 498 cases (40.5%) were anemic, mainly of the mild type; 208 anemic children (41.8%) had no hemoglobinopathies, 140 (28.1%) had hemoglobinopathies and 150 (30.1%) were not tested for hemoglobinopathies. The commonest type of hemoglobinopathy was alpha-thalassemia, 91 (18.5%), followed by sickle cell trait, 58 (11.6%). 224 of the mothers of anemic infants (45%) had no anemia and 218 (43.8%) were anemic. Overall, 338 mothers with anemic infants (76.4%) had no hemoglobinopathies.
Conclusion: Anemia among infants is decreasing in the Kingdom of Bahrain generally and decreasing with age specifically but it is still considered a severe public health problem. Most of the cases of anemia among nine-month-old children are due to iron deficiency anemia and one-fifth of the cases are hemoglobinopathies. It is recommended that iron drops be supplied as daily dietary supplementation at weaning and to be continued for one year for those with negative sickle cell disease and thalassemia test at birth.
Keywords: prevalence of anemia; child screening services; hemoglobinopathies; Bahrain
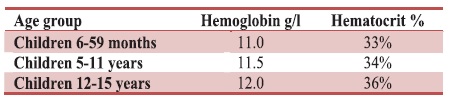
Anemia is a condition in which the body does not have enough healthy red blood cells due to a decreased concentration of hemoglobin and red blood cell mass.1 According to the World Health Organization, anemia in children is based on age specific cut-off levels of hemoglobin. See Table 1.2
Table 1. Cut-off levels for anemia based on WHO criteria
Globally, anemia affects 1.62 billion people which corresponds to 25% of the world’s population and the higher prevalence is among preschool-age children, 47.4%, ranging from 64.6% in Africa to 3.4% in North America; it is lowest in men, 12.7%.3 Iron deficiency anemia ranks number nine among 26 risk factors in the Global Burden of Disease (GBD) and accounts for 841,000 deaths and 35,057,000 disability-adjusted life-years lost.4
Iron deficiency anemia contributes to poor cognitive development, increased maternal mortality and decreased work capacity. It is caused by iron-poor diet, rapid growth (in the first year of life and in adolescence), or the inability of the body to absorb iron such as with cow’s milk. Iron deficiency anemia during pregnancy adversely affects the iron level of the infant at birth. In the first 6 months of age, iron stores are dependent on what has occurred during pregnancy. The fetus extracts iron in amounts proportional to the levels available in the mother. Infants of mothers with moderate and severe anemia have significantly lower cord serum ferritin levels and poor iron stores at birth. Iron deficiency commonly develops after six months of age if the complementary foods do not provide sufficient absorbable iron, even for exclusively breastfed infants.5 Another cause of anemia in infants is hemoglobinopathies, inherited variants in a recessive gene that involves the synthesis of a portion of adult hemoglobin (hemoglobin A). The World Health Organization estimates that at least 5% of adults globally are carriers for a hemoglobin condition, 2.9% thalassemia and 2.3% for sickle cell disease. Other causes of anemia are rare.6
In Bahrain, all infants have their hemoglobin level checked at nine months of age. Using the hemoglobin level as an indicator, 48% of children under five years of age were found to be anemic and 60% of infants 6-9 months of age were anemic according to a study done in 1995,7 while a national estimate of anemia (1993-2005) showed 24.7% of preschool children had anemia,3 but recent annual statistics of 2012 showed that anemia dropped to 31% in same age group. However, it is still considered a moderate public health problem.
To address this public health problem and to provide a clear and simple recommendation for prevention and treatment of anemia in children, this study was done to estimate the prevalence of anemia among nine-month-old infants attending child screening services in local health centers all over the Kingdom during the month of July 2012 and to describe the impact of hemoglobinopathies and the relationship of anemia in mothers during pregnancy to anemic infants.
All nine-month-old infants born in September 2011 that visited screening services in Primary Health Care during July 2012 and had their hemoglobin levels tested were included in the study. Testing of hemoglobin at nine months of age is recommended by the National Child Screening Guidelines in Bahrain, which is similar to the recommendations of the Centers for Disease Control (CDC), United States Preventive Services Task Force (USPSTF), the American Academy of Family Physicians and the American Academy of Pediatrics which have recommended that all infants at high risk for iron deficiency anemia be screened between 9 and 12 months of age regardless of blood lead level.8
Hemoglobin level is tested by finger prick using a hemoglobin meter (Hem cue machines) in local health centers. The child is considered anemic if his/her hemoglobin level is below 11 g/dl. The result of hemoglobin electrophoresis, collected from cord blood at birth as part of the national newborn screening program, is usually taken from the child screening booklets or the electronic laboratory system using the temporary personal card of the infant or telephone number of either of the parents.
Information about the mothers was taken from the Mother and Child Health Oracle system and the electronic laboratory system is used to get the last hemoglobin level done during pregnancy and hemoglobin electrophoresis of the mother. The mother is considered anemic if her hemoglobin level during pregnancy is less than 11 g/dl.
The study included all twenty-two governmental health centers, i.e. all the health centers that provide mother and child health services in the Kingdom of Bahrain. Governmental health centers in the country give care to around 70% of the population.
1,378 records for nine-month-old children were studied, 1,230 had hemoglobin level (Hb) test done (89.3%) of which 498 cases were anemic (40.5%). Gender distribution among anemic patients was: male 224 (45%) and female 274 (55%).
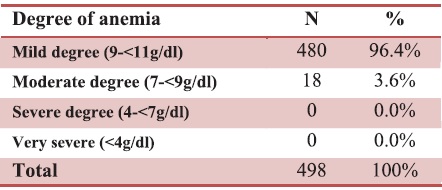
Table 2 shows that the majority of anemic cases are of a mild degree and some are of moderate degree of anemia. None of the cases attending the child screening services in the health centers had a severe degree of anemia.
Table 2. Degree of anemia among nine-month-old children attending child screening services
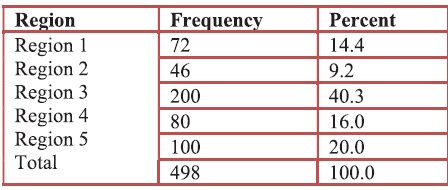
Among the five regions in the Kingdom of Bahrain, region three had the highest number of anemic cases (see Table 3).
Table 3. Distribution of anemia in nine-month-old children based on regions
Of the 498 anemic cases 348 had hemoglobin electrophoresis test done, the results showed that 208 (41.8%) of anemic children had normal hemoglobin electrophoresis, 140 (28.1%) had hemoglobinopathies and for 150 (30.1%) the blood results were not available.
Table 4. Hemoglobinopathies results among anemic cases

The commonest types of hemoglobinopathies were alphathalassemia (67, 13.5%) followed by sickle cell trait (SCT) (35, 7%). The mixed type of hemoglobinopathy cases were 25 (5%) (all mixed type were alpha-thalassemia with 2 cases of sickle cell disease (SCD) and 23 cases of SCT). Beta-thalassemia trait was 1.4% and hemoglobin E only 0.2% (see Table 4). Of the total anemic children, 224 (45%) of their mothers had no anemia, 218 (43.8%) were anemic. Among the anemic mothers, 163 had no hemoglobinopathies. Overall, 338 (76.4%) of mothers with anemic infants had no hemoglobinopathies (see Figure 1).

Figure 1. Hemoglobin level test: mothers
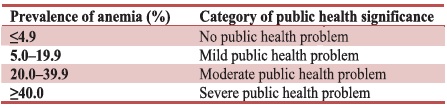
Anemia in infants is a frequent laboratory result challenging general medical doctors in primary health care, even though studies indicate that the percentage of anemia is decreasing in the Kingdom it is still high as seen in this study, it reached 40.5% which is considered a severe public health problem using the WHO population-specific hemoglobin classification (see Table 5).
Table 5. WHO category of public health significance of anemia
Studies have shown that the prevalence of anemia in the Arab Gulf countries is high, ranging in preschool children from 20-67% and among school children from 13-50%, using hemoglobin level as indicators.9
In comparing the problem with other countries, the level of anemia in Bahrain is as high as it is in the other Arab Gulf countries but it is higher than in the United States of America where the average prevalence of iron deficiency anemia in infants 1–2 years is 6 to 17 per 1000.10 In southern Iran the prevalence of iron deficiency anemia was found to be 19.7% in children between 6 months and 5 years of age.11 In Oman, the prevalence of anemia among preschool children was 42%. Anemia prevalence was significantly higher in children under 2 (66%) compared to those 2-5 years of age (26%).12
Another significant finding in MCH statistics for 2012 was that infants at nine months of age had an anemia prevalence of 31%. It decreased gradually with age reaching 17.7% at 18 months and 4.23% at school entry, similar to findings of an old study done in 19957 in southern Iranian children.11 This could be due to treatment and better diet intake with increasing age. This also raises the issue whether to start iron drops at weaning for all children at 6 months with negative hemoglobinopathy test at birth for about one year.
Regarding hemoglobinopathies, the frequency of betathalassemia in Bahrain was found to be low to moderate compared with other Gulf countries such as the UAE, Qatar and Kuwait. Sickle cell disease (SCD) is more common than beta-thalassemia in Bahrain, the incidence of SCD affecting newborns was found to be 0.7% in 2008, 0.6% in 2009, and 0.4% in 2010. A study among secondary school students in Bahrain from 1999-2008 showed that the mean prevalence of the beta-thalassemia trait and major were 3.5% and 0.032%, respectively.13-15
A study of hemoglobinopathies in Oman through a national register showed that 10% had sickle cell anemia and 4% had beta-thalassemia major. Another survey in Oman revealed that hemoglobinopathies are prevalent in Oman; the prevalence of sickle cell trait was 6%, and of beta-thalassemia 2%. The prevalence of sickle cell and homozygous beta-thalassemia were 0.2% and 0.07%, respectively.16
A survey done in Qatar using the results of all hemoglobinelectrophoresis performed in a hematology laboratory at Hamad Hospital for Qatari residents revealed that 16.33% were found to carry a structurally abnormal hemoglobin variant of one type or another, and 14.63% had sickle cell hemoglobin.17 In southern Iran the prevalence of sickle cell trait and sickle cell anemia has been estimated to be around 1.43% and 0.1%, respectively, beta-thalassemia has a high prevalence (around 10%) in the north.18
Excluding the unavailable results, most of the infants in our study can be treated with iron drops. In addition to iron drops supplementation, fortifying weaning food is needed as the iron demand is less than the iron intake.
Another less common cause of anemia is lead poisoning. Both the Centers for Disease Control and Prevention (CDC) and the American Academy of Pediatrics (AAP) recommended that all children have their blood lead concentration measured at between 1 and 2 years of age.19
The national program for newborn screening for hemoglobinopathies and hypothyroidism is done for all newborns delivered in governmental hospitals by testing cord blood at birth. In this study 30% of the results were not available, either due to not merging the temporary identification number at birth with the permanent identification number or screening was not done.
Anemia is a problem frequently seen among pregnant mothers. Studies in the Gulf countries have shown that iron deficiency anemia is a serious public health problem among pregnant women, the prevalence ranging as high as 54% in Bahrain to the lowest in the region in Qatar around 30%.20 In Bahrain, 33.5% of pregnant women were anemic and 40% of them had iron deficiency anemia according to a survey done in 1995,21 while in 2003, 51% of women of childbearing age had anemia and 25% had iron deficiency anemia.7 Recent statistics in 2012, showed that out of 12,750 mothers, 27.8% had anemia at booking. Many studies showed that maternal anemia can cause anemia in their infants, a prospective study in Jordan showed a significantly higher anemia in infants born to anemic mothers (81%) compared to controls (65%).22
In this study, 44% of the mothers of anemic infants were anemic but this requires further investigation especially as the control group of non-anemic infants was not included in the analysis.
Although studies have shown that anemia among children is decreasing in the Kingdom of Bahrain generally and decreasing with age specifically, it is still considered a severe public health problem. More efforts should be made to prevent anemia at 9 months. As most of the cases of anemia among 9-month-old infants are due to iron deficiency anemia and one-fifth only is due to hereditary untreatable hemoglobinopathies, the following recommendations are suggested: