
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2014, Volume 25, Issue 2, Pages 71-74
http://doi.org/10.26715/jbms.25_2_2Hind Al-Sindi,* Mazen Al-Mulla,* Amina Bu-Saibaa,* Bushra Al-Sharaf,* Jaleela S. Jawad,** Osama A. Karim,***
*Family Physician, Primary Care, Ministry of Health, Kingdom of Bahrain
**Family Physician, Public Health Directorate, Ministry of Health, Kingdom of Bahrain
***Consultant Pediatric Pulmonologist, Salmaniya Medical Complex, Ministry of Health, Kingdom of Bahrain
Correspondence to: hind_md@hotmail.com, osama_ka@hotmail.com, jalila517@hotmail.com

Objective: To estimate the prevalence of asthma, rhinitis and eczema symptoms in school children aged 6-7 years.
Design: A cross-sectional study of randomly selected primary schools for children.
Setting: Government and private primary schools in Bahrain.
Method: A standardized ISAAC-validated Arabic-translated questionnaire was distributed to 3,000 students aged 6-7 years in 18 primary schools which was to be completed by parents or guardians.
Results: 1,951 questionnaires were completed. Participants included 1,094 males (56.1%) and 857 (43.9%) females. The prevalence of asthma was 10.8%, allergic rhinitis, 16.5% and eczema, 9.8%. The prevalence rates for physiciandiagnosed asthma were greater in males 13.3% than females 8.7% [CI (1.8-7.4)]. Symptoms of sneezing or blocked nose showed male gender predominance (18.3%) in comparison to females (14.2%) [CI (0.77-7.5)]. Ever diagnosed hay fever also followed the same pattern of a male predominance of 5.4% in comparison to 3.3% in females [CI (0.24-3.9)]. Female predominance was found in prevalence of itchy rash, 12.5% in comparison to males (8.5%) [CI (-6.9 to -1.2)]. 58.6% had symptoms of allergic rhinitis with a significant peak in the winter season [CI (50.9-66.3)], only 11.2%, had symptoms in the summer season [CI (6.48-16.4)].
Conclusion: Prevalence of asthma, rhinitis and eczema symptoms found in this study were all similar to those reported in other Gulf neighboring countries; with a significant male predominance found in asthma and rhinitis, but not in atopic eczema.
Allergic diseases have become a global public health problem. The increased prevalence of allergy is such that currently between 20–30% of the world’s population suffers from some form of allergic disease1. It is estimated that more than 80 million people in Europe suffer from some kind of allergic disease, and that by 2015 half of all Europeans will be similarly affected. Nevertheless, asthma and other allergic diseases are still considered underdiagnosed and under-treated, creating a substantial burden on individuals and families with significant impact on quality of life.
Many countries around the world have followed the International Study of Asthma and Allergies in Childhood (ISAAC) protocol, whose main objectives are to continue to measure symptom prevalence and severity of asthma, rhinitis and eczema in children, especially in developing countries where prevalence of the conditions has not been documented3.
The ISAAC phase I protocol is structured to identify the symptom prevalence of asthma, rhinitis and eczema. This was done in almost 2 million children in 106 countries all around the world 3. The ISAAC phase I protocol studied the prevalence of asthma, rhinitis and eczema in school children aged 6-7 years through a standardized questionnaire filled in by parents or guardians with the addition of a selfadministered video questionnaire for children aged 13-14 years3.
In the last couple of years many Middle Eastern countries and all of the Gulf countries have adopted the ISAAC protocol, including Saudi Arabia, Kuwait, Qatar, UAE and Oman4-7. The objective of this study is to provide baseline data which can be used for further planning and management of childhood asthma and allergic diseases in Bahrain, based on the ISAAC phase I protocol.
This cross-sectional study was carried out from June 2010 to July 2010 on children aged 6-7 years in 18 primary schools in the Kingdom of Bahrain.
A list of all primary schools both government and private was obtained from the Ministry of Education. The lists were serially numbered; schools were selected by systematic random sampling, after which a number were selected by using a table of random numbers. 18 primary schools were selected and a proportionate number of each school’s students aged 6-7 years (grades 1 and 2, of both private and government) were selected to reach a total of 3,000 students. Approval was granted from the Ministry of Education to distribute the questionnaires to be filled in by parents or guardians of the students.
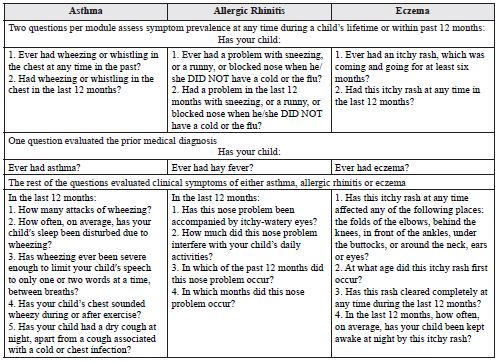
A standardized ISAAC phase I-validated Arabic-translated questionnaire was used after permission was granted from the authors of the Kuwait ISAAC study8. A summary of the questionnaire is shown in Table 1:
Table 1. A summary of the ISAAC core questionnaire module for asthma, allergic rhinitis and eczema for children aged 6-7 years
 A brief definition in Arabic of hay fever was provided at the end of the questionnaire and a hotline number was provided where an asthma-trained nurse stood by prepared to answer any enquires about any of the questions to ensure full understanding of the questionnaire. Data was entered and analyzed using SPSS 11.0 package. Descriptive statistical analysis included frequencies for categorical data. Proportionate calculations and confidence interval (95% CI) were calculated.
A brief definition in Arabic of hay fever was provided at the end of the questionnaire and a hotline number was provided where an asthma-trained nurse stood by prepared to answer any enquires about any of the questions to ensure full understanding of the questionnaire. Data was entered and analyzed using SPSS 11.0 package. Descriptive statistical analysis included frequencies for categorical data. Proportionate calculations and confidence interval (95% CI) were calculated.
From the total number of questionnaires distributed to 3,000 students aged 6-7 years throughout different schools in the five governorates of Bahrain, a response rate of 65% was achieved with a total of 1,951 questionnaires returned, 56.1% of the respondents were male students and 43.9% were females. The overall prevalence rates for wheeze ‘ever’ and physician-diagnosis of asthma was 204/1,892 (10.8%) [CI (9.38-12.2)], and 216/1,917 (11.3%) [CI (9.85-12.7)] respectively (See Table 2). The prevalence rates for wheeze ever and physician- diagnosed asthma were greater in boys 147/1,071(13.1%), than girls 73/841(8.7%) and the differences were statistically significant (p=0.009 [CI (0.98-06.5)] and 0.002 [CI (1.8-7.4)] respectively (See Table 3).
Table 2. The prevalence of self-reported symptoms and diagnosis of asthma, rhinitis, and eczema in 6-7 year-old children
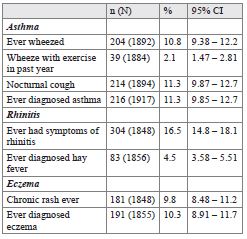
The overall prevalence rate for sneezing or blocked nose ever was 304 (1,848), or 16.5% [CI (14.8-18.1)]. Symptoms of sneezing or blocked nose also showed male gender predominance, 18.3%, in comparison to females with the same symptoms 14.2% (p value=0.018 and [CI (0.77-7.5)]) (See Table 3). The prevalence rates for itchy rash ever were 181 (1,848), or 9.8% [CI (8.48-11.2)]. Nevertheless, only 191 (1,855), or 10.3% [CI (8.91-11.7)] of the total population of children had a diagnosis of eczema by a physician; with females predominant, 102 (813), or 12.5%, in comparison to males 88 (1,037), or 8.5%, with a p value 0.004 and [CI (-6.9 to -1.2)] (See Tables 2 and 3).
Table 3. The prevalence of self-reported symptoms and diagnosis of asthma, rhinitis, and eczema in 6-7 year-old children in Bahrain in relation to gender
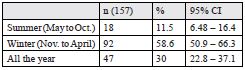
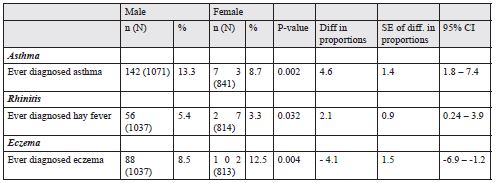 It was found that symptoms of allergic rhinitis showed a significant winter seasonal peak of 92/157 (58.6%) [CI (50.9-66.3)], whereas prevalence in the summer season was 18/157 (11.2%) [CI (6.48 – 16.4)] (See Table 4). The results revealed that the overall prevalence rate of diagnosed hay fever was 83/1,856 (4.5%) with predominance in the male population 56/1,037 (5.4%), in respect to female being 27/814 (3.3%) [CI (0.24-3.93)] (See Tables 2 and 3).
It was found that symptoms of allergic rhinitis showed a significant winter seasonal peak of 92/157 (58.6%) [CI (50.9-66.3)], whereas prevalence in the summer season was 18/157 (11.2%) [CI (6.48 – 16.4)] (See Table 4). The results revealed that the overall prevalence rate of diagnosed hay fever was 83/1,856 (4.5%) with predominance in the male population 56/1,037 (5.4%), in respect to female being 27/814 (3.3%) [CI (0.24-3.93)] (See Tables 2 and 3).
Table 4. Seasonal distribution of allergic rhinitis symptoms
The asthma prevalence rate reported in this study is within the range found in other studies from neighboring Gulf countries; 11.4% in Saudi Arabia, 10.5% in Oman and 13.6% in UAE6, 10, 11. Qatar showed a higher prevalence rate than other Gulf countries of 21.9%. This could be explained by the use of an additional method (video) whereas other countries have used only the selfadministered questionnaire5. The similarity of the results in other studies across the countries in the Gulf region, may be due to the similarity in factors such as population distribution, cultural, environmental, ethnic, geographical and socio-economic status, the same factors that may cause variations in the results of asthma prevalence studies from other countries.
Despite the relatively low response rate in our study, it was considered that it did not affect the results since it approximated that found in neighboring Gulf countries. It was also considered that even if the non-respondents were added to the results it would not change the results because of the similar characteristics of the respondents in this study. Data shows that the prevalence rates of physician-based diagnosis of asthma were greater in boys than girls, thereby indicating that gender difference is a consistent finding and also similar to findings reported in other countries such as Oman, Iran, Hong Kong, United Kingdom, and New Zealand6, 9, 12-14. It was also noted that the prevalence rate of physician-based diagnosis of asthma is higher than the prevalence rate of those who had wheeze ever. This finding was similar to that found in Oman, however contradicting the findings of the ISAAC study done in Urmia in Northern Iran, which showed under- diagnosis of asthma6, 9.
The prevalence of sneezing and blocked nose fall within the range of the neighboring Gulf countries: in Qatar 30.5%, Oman 7.4% and KSA 12.7%5, 6, 13. Symptoms of allergic rhinitis peaked during the winter season; this may be attributed to an increase in the incidence of viral upper respiratory tract infections that may initiate or overlap with the symptoms of sneezing and blocked nose or their confusion between common cold symptoms and allergic rhinitis15. Bahrain’s climate may have also contributed to the winter peak, since it is categorized into two seasons, summer and winter16. The latter includes the spring season (March to April), where pollen allergy may also initiate symptoms of allergic rhinitis. This was supported by a study that concluded that the indigenous trees of Middle Eastern countries, such as date palms, acacia and mesquite, have a specific pollen season (from March to May) that is suggestive of an aero-allergenic origin15. Furthermore, our findings were consistent with other studies where results showed a peak prevalence in the winter season, such as Thailand and New Zealand14, 17.
Similar to the higher male prevalence found in asthma, a male predominance was also seen over females in both prevalence of allergic rhinitis and hay fever. This male gender predominance was also found in neighboring countries, such as Oman, Qatar and Iran5, 6, 9. Furthermore, the same high proportion of males was also noticed in Western countries for example Hungary18. Prevalence of hay fever in our study also falls within the range of other Middle Eastern countries, such as Iran 3.6%9, Oman 7.5%6 and 14.9% in UAE12.
The prevalence of itchy rash ever and physician diagnosed eczema were very close and almost identical. This can be explained by the knowledge of the general population that itchy rash in certain flexural areas is the main feature to the diagnosis of eczema. Furthermore, this prevalence also was similar to that found in other GCC countries (UAE 11%, Qatar 22.5%, Oman 7.5%, and KSA 13%)5, 6, 10, 11. The study also showed significant difference in prevalence of physician-diagnosed eczema in relation to gender. Unlike the male predominance noted in asthma and allergic rhinitis, female gender predominates in atopic eczema; this finding is in parallel with the findings reported in the region (Qatar, Iran and Oman)5, 6, 9.
Another important unique aspect of this study is the questionnaire-related enquiries received by the asthma trained nurse from the children parents. She received around 30 phone calls during data collection; most of these required further clarification of the term “hay fever” despite having been provided with the definition. Some enquiries sought clarification of the characteristics of the rash. All enquires were answered and the nurse welcomed any further questions.
The prevalence of asthma, allergic rhinitis and eczema in children aged 6-7 years was 10.8%, 16.5% and 9.8% respectively. All of which were similar to the prevalence found in neighboring Gulf countries. Furthermore, significant male gender predominance was noted in asthma and allergic rhinitis while a higher percentage of female gender is seen in atopic eczema.