
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2018, Volume 30, Issue 2, Pages 47-53
https://doi.org/10.26715/jbms.2_30082018Amal Abbas1, Batool Al Nawah1, Fatema Makhlooq1, Zainab Hubail1, Amani Al Hajeri2*
1Family Physician, Ministry of Health, Juffair, Kingdom of Bahrain.
2Consultant Family Physician, Consultant Clinical Geneticist, Head of Genetic Department, Salmaniya Medical Center, Ministry of Health, Juffair, Kingdom of Bahrain.
*Corresponding author:
Amani Al Hajeri, Consultant Family Physician, Consultant Clinical Geneticist, Head of Genetic Department, Salmaniya Medical Center, Ministry of Health, Juffair, Kingdom of Bahrain; Tel: (+973) 17284490, Email: alhajeriamani@gmail.com
Received date: April 18, 2018; Accepted date: August 30, 2018; Published date: September 21, 2018

Background and objectives: Complementary food patterns play a fundamental role in infant growth and health, especially in the first two years of life. This study aimed to explore the pattern and practice of complementary feeding of infants in Bahrain.
Methods: A cross-sectional study, including 364 children attending the primary healthcare clinics in four primary health centers was conducted in Bahrain. A pre-tested structured questionnaire, including a one week recall food frequency was administered. Data was collected via face to face interview with caregivers.
Results: Of the 364 caregivers interviewed, only 56% followed the recommendation of introduction of food at the age of six months, whereas, 41.8% caregivers followed the recommended number of meals at the age of nine months. Mothers experience was associated with complementary food introduction age (P < 0.008).
Conclusion: The pattern and practice of complementary feeding in Bahrain is not meeting the WHO recommendations.
Keywords: Complementary feeding, age of introduction, meal frequency, malnutrition
According to the recommendations of World Health Organization (WHO), complementary feeding should start at the age of six months.1 The food should be given in a gradual manner in order to introduce a variety of food groups by the age of nine months. The transition from exclusive breast feeding to external food, referred to as complementary feeding, typically covers the period between six and 24 months of age.1 It is the time when malnutrition starts in many infants, contributing significantly to the high prevalence of malnutrition in children less than five years of age, worldwide. According to WHO,2, 3 in many countries only one third of the breastfed infants between six and 23 months of age meet the criteria of dietary diversity and feeding frequency that are appropriate for their age.
Complementary food should be given in certain amounts, frequency, consistency, and using a variety of food to cover the nutritional needs of the growing child, while maintaining breast feeding.2, 3 The WHO recommends exclusive breast feeding up to six months of age and introduction of complementary foods at six months, while maintaining breastfeeding on demand to two years of age or beyond. Meal frequency should be 2–3 times per day at 6–8 months of age and 3–4 times per day during 9–11 months of age.2, 3
Studies from various parts of the world, such as the Lebanese Republic, India, Ethiopia, and Iran have suggested that widespread education regarding the initiation of complementary feeding is required. It will aid in behavioral change, and communication activities should be implemented in the maternal and child health unit of the hospitals.4-8
In Bahrain, children are followed up regularly in healthcare clinics for children, from birth throughout childhood. Physicians advice regarding the importance of exclusive breastfeeding until the age of six months and the right age to start complementary feeding. At the age of six months, caregivers are instructed about the dietary routine and a complementary feeding booklet is provided.
Therefore, the study was conducted to assess complementary feeding at the age of nine months, which is the earliest visit after the age of six months i.e. after the course of breastfeeding. The aim of the study was to evaluate the pattern and practice of complementary feeding in infants at the age of nine months in Bahrain in order to improve the nutritional status of the children.
A cross-sectional observational study was conducted among children aged 9–24 months attending the Maternal Child Health Unit in primary healthcare centers in Bahrain. Our sample was taken from the registry of health information department of the Ministry of Health population statics. The researchers chose a convenient sample of 364 children out of a total of 19875 children aged 9–24 months, according to the health statistics in the Ministry of Health.
Caregivers of children aged 9–24 months attending the child health unit in the primary healthcare center were included in the study, regardless of nationality and health status of the child. Children with chronic diseases, such as asthma and sickle cell disease were included since the recommendations do not differ. Non-English or non-Arabic speaking caregivers and infants not present with their primary caregivers were excluded from the study.
Verbal informed consent was obtained from each study participant after explaining the purpose and procedure of the study. All the study participants were reassured regarding the confidentiality of their identification. Ethical approval was obtained from the Ethical Committee of Ministry of Health, Bahrain.
To calculate the sample size, we used an equation that required an estimated prevalence of complementary feeding practices among children worldwide. Worldwide, complementary feeding practice error was estimated to be around two-third, according to the WHO. The calculated number was estimated to be 342. One health center was selected randomly from each health region in the Kingdom of Bahrain by simple random sample using a computer system.
A self-piloted constructed questionnaire was used to interview the caregiver. The questionnaire included four sections: first section—demographic data, including child age, gender, nationality, number of children in the family, and educational level and working status of mother and father; second section—complementary feeding practices, such as who encouraged initiation and the source of information about complementary feeding; third section—complementary feeding recommendations, including timing of introduction of solid food, number of meals at nine months, and food administered gradually or together; fourth section—age of introduction and frequency of food (cereal, fruits, vegetables, fish, chicken, meat, legumes, dairy products, and eggs).
Data was entered and analyzed using SPSS 20. Frequencies and percentages were computed for categorical variables, whereas mean and standard deviation were computed for the quantitative variables. Cross-tabulation was done between two categorical variables. Chi-square test was used to determine significant relationship between two categorical variables; P ≤ 0.05 was considered statistically significant.
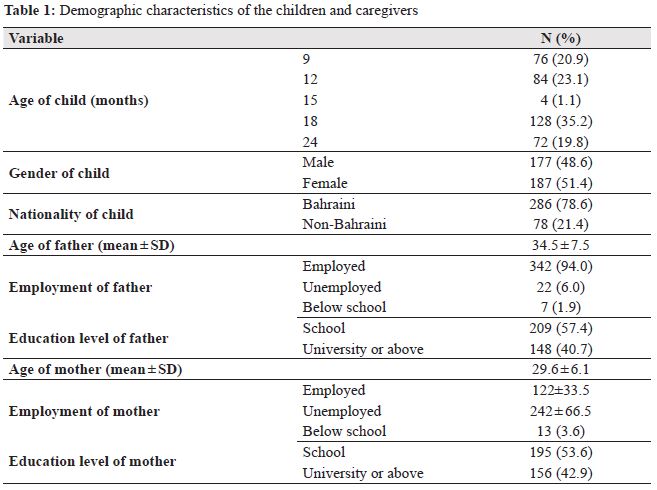
The demographic characteristics of the study group are given in Table 1. The common age of children was 18 months (35.2%). The majority (78.6%) of the population were nationals of Bahrain. The mean age of the mothers and fathers were 29.6 ± 6.1 years and 34.5 ± 7.5 years, respectively. The percentages of employed fathers and mothers were 94% and 33.5%, respectively. Almost equal percentage of fathers and mothers were educated, with most of them completing only schooling (57.4% vs. 53.6%, respectively).
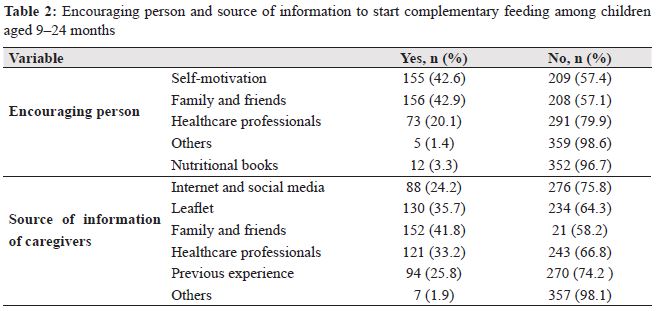
In our sample, it was identified that caregivers were encouraged to start complementary feeding in different ways: 42.9% were encouraged by friends and family and 42.6% were self-motivated to start complementary feeding. The contribution of health care professionals was only 20.1%. The source of caregiver’s information about complementary feeding was from internet and social media (24.2%), family and friends (41.8%), and health care professionals (33.2%; Table 2).
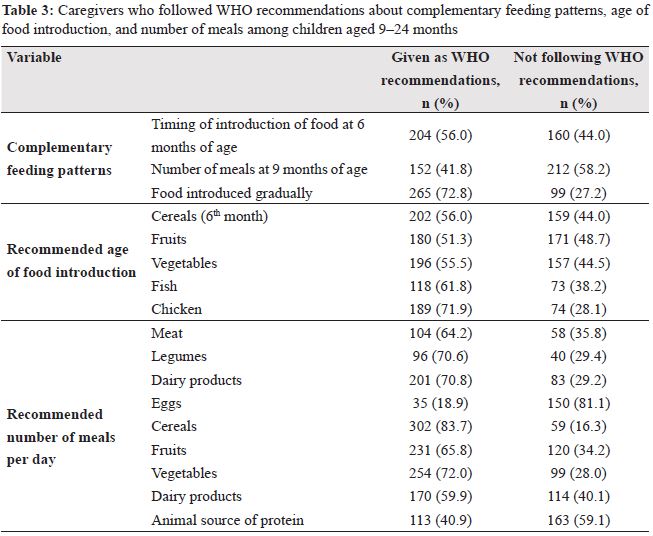
 Out of the 364 caregivers interviewed, 56% followed the recommendation of introduction of complementary feeding at the age of six months and 41.8% caregivers followed the recommended number of meals at the age of nine months (Table 3). Mothers experience was significantly associated with the age at which complementary feeding was introduced (P < 0.008; Table 4).
Out of the 364 caregivers interviewed, 56% followed the recommendation of introduction of complementary feeding at the age of six months and 41.8% caregivers followed the recommended number of meals at the age of nine months (Table 3). Mothers experience was significantly associated with the age at which complementary feeding was introduced (P < 0.008; Table 4).
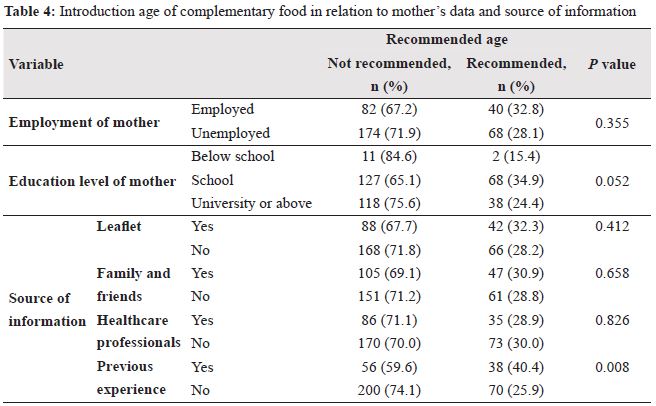
Significant association was not observed while comparing the mother’s working status with the introduction of complementary feeding at the recommended age. However, the educational level of the mother plays a crucial role (P = 0.052). Mothers with previous experience were significantly better in following the recommendation when compared to unexperienced mothers (P = 0.008; Table 4).
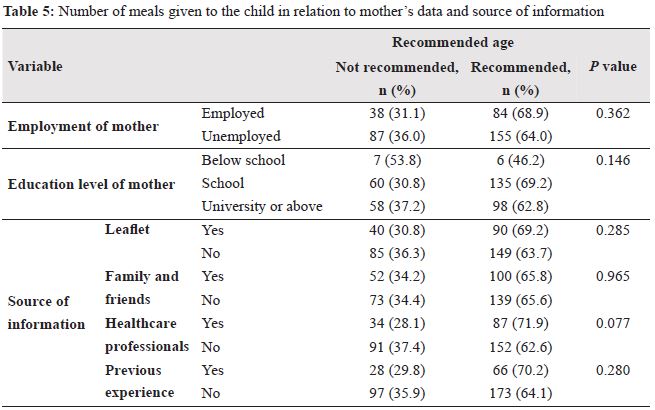
There is no significant relationship between the number of meals consumed by the children and working status of the mother, educational level of the mother, and the source of information (Table 5).
 Discussion
DiscussionThere is a dearth of studies conducted in this respect in the Gulf countries; therefore, studies from the Middle Eastern countries, such as the Lebanese Republic and Iran were used.
In the present study the lowest (1.1%) percentage of participants were observed at the age of 15 months, as this age group was included recently in the vaccination schedule, July 2015. In this study most of the participants were encouraged to introduce complementary feeding by the family, friends, and through self-motivation. The role of health care professionals was disappointing. Initiation of complementary feeding should be discussed with caregivers, failure to do so might be due to focus on other points during the visit and lack of time.
The sources of information were family/friends, leaflets, and health care professionals. In a study conducted by Kwalzulu et al.,6 62% caregivers received information from the community health workers and 33% from clinics, whereas, 22% did not receive information. Initiation of communitybased health care program helped in spreading the information in their community.
In our sample 56% started weaning at 6 months of age. Compared to Lebanon, it was much higher, starting at the age of 4 months according to their regional guidelines.5 In other parts of the world like India and Kwalazulu it was comparable, 40% and 39% respectively.6, 7 In our sample the reason for caregivers not following-up was due to following the old recommendations at the age of four months, previous experiences, due to lack of knowledge, and the misconception that the baby will not accept food later. Some communities later believed that the baby might not tolerate the food. Even in the Mediterranean and Gulf regions complementary feeding was initiated early when compared to developing countries, such as India and Kwalazulu, which are influenced by their economic level depending more on breastfeeding leading to late weaning.
In the Lebanese Republic, more than 90% of children were given cereals, fruits, vegetables, dairy products, eggs, meat, and legumes, showing a greater lag of practice in our region.5 Reasons might be allergy due to eggs, child refusal to eat, mother impatience, lack of knowledge, or other reasons.
On the other hand, the percentage who followed the recommendation of frequency of meals in the Lebanese Republic was 57.1% for bread, 52% for biscuits,65.8% for fruits, 21.8% for chicken, 61.5% for lamb, 32.1% for beef, and 50.8% for fish, which shows less protein administered.5
The working status of mothers had no effect on the age of introduction of complementary feeding, while the mother’s educational level played a slightly significant role. In the Lebanese Republic it was affected by employment and educational level as working mothers and mothers with higher educational level started weaning earlier. In the Kingdom of Bahrain, most information is gathered from family and friends who are not necessarily following the guidelines. Many grandmothers are taking care of children of working mothers, hence still following the old guidelines of weaning at the age of 4 months.5
The source of information showed no significant association in relation to the age of introduction of food among the different sources, except for mothers with previous experience as they showed more adherence to the timing of weaning.
The sample in the present study was a convenient sample, which raised the issue of selection bias.
The pattern and practice of complementary feeding in the Kingdom of Bahrain does not meet the WHO recommendations.
The role of health care professionals in encouraging the initiation of complementary feeding and providing information to the caregivers was poor. We recommend that education should be started at the visit of caregivers after 4 months with the assistance of dietitians or health educators.
The role of health care professionals should be continued throughout the subsequent child visits. The types, amount, frequency, and consistency should be reviewed at each visit and individualized; appropriate advice should be provided.
There are various wrong believes regarding the time of introduction of each type of food, hence, the complementary feeding booklets need to be updated.
Further, studies aiming to target complementary feeding practice among larger group and wider range of age are recommended, including food practices and safety and other aspects of complementary feeding. Emphasis on food safety and preparation and a larger sample size, with concentration on nine-month-old children are recommended.
The authors of the study have no conflict of interest to declare.