
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2018, Volume 30, Issue 3, Pages 25-33
https://doi.org/10.26715/jbms.3_2512a2018Shooq Alsooreti1*, Batool Alalawi2, Hesa Abdulkarim1, Sara Mohamed1, Wafa AlSharbati3
1Medical Doctor, MD, Primary Care Physician, Bank Bahrain and Kuwait Hid Health Centre, Kingdom of Bahrain
2Medical Doctor, MD, Primary Care Physician, Al Dair Health Centre
3Medical Consultant, Primary Care Consultant, Public health Consultant, Public Health Directorate, Ministry Of Health
*Corresponding author:
Shooq Alsooreti, Medical Doctor, MD, Primary Care Physician, Bank Bahrain and Kuwait Hid Health Centre, Kingdom of Bahrain; Tel: (+973) 36195556, Email: Alshoooq_16@hotmail.com
Received date: August 10, 2018; Accepted date: December 25, 2018; Published date: December 31, 2018

Background and objectives: Worldwide, mortality due to cardiovascular diseases (CVD) is a concern of great magnitude. The mortality rate in Bahrain, due to CVD, was 19.5%, 32%, and 21.5% in the years 2005, 2011, and 2013, respectively. The objective was to assess the awareness of Bahraini adults of the early warning symptoms of heart attack (HA) and the need to activate rapid emergency care by calling 999 once recognized.
Methods: An observational cross-sectional study included 400 Bahraini adult patients attending primary healthcare centers in Bahrain. Respondents were asked to identify the five warning symptoms of a HA and the first action to be performed while witnessing a HA. HA knowledge score was calculated for each respondent. The study was approved by Bahrain Public Health Research Committee.
Results: Based on the evaluation of the knowledge scores of HA symptoms, 71.9% and 28.1% of the participants scored poor and good level of knowledge. In the study, the most recognized symptom of HA was chest pain (70.9%) followed by shortness of breath (60%). In response to the first action to be performed while witnessing a HA, only 59.5% reported that they would contact the emergency services.
Conclusion: The level of public awareness about HA symptoms in Bahrain is poor. Community campaigns are required to increase public health knowledge.
Keywords: Chest pain, Heart attack, Knowledge, Public awareness, Symptom
Cardiovascular disease (CVD) is the “group of disorders of heart and blood vessels, and includes: hypertension, coronary heart disease, cerebrovascular disease (stroke), peripheral vascular disease, heart failure, rheumatic heart disease, congenital heart disease, and cardiomyopathies”.1
Globally, CVD related death is a concern of great magnitude. In 2012, the World Health Organization (WHO) had estimated a mortality rate of 17.5 million due to CVD, representing 31% of all global deaths.1 Of these deaths, an estimated 7.4 million were due to coronary heart disease. The WHO estimates 23.6 million CVD deaths in 2030.2 The mortality rate in Bahrain, due to CVD, was 19.5%, 32%, and 21.5% in the years 2005, 2011, and 2013, respectively.3, 4
Symptoms of myocardial infarction (MI), commonly known as a heart attack (HA), may be immediate or may start slowly and persist for hours, days, or weeks before death occurs.5The longer an individual is not treated, the greater the damage. The five major warning signs and symptoms of HA are: pain or pressure in the chest; pain or discomfort in the jaw, neck, or back; lightheadedness or fainting; shortness of breath; and pain in the shoulders or arms.6The American Heart Association recommends calling the emergency response number as the first action to be done even if not sure of witnessing a HA.5
The prehospital delay occurs due to reduced knowledge of the patients that these symptoms need urgent medical care and sometimes may recognize the symptoms but do not know where to go first. The reason for this is possibly due to insufficient knowledge of the warning signs of a HA. However, increasing awareness among the population can prevent delay in treatment.7
In this study, we assessed the level of awareness of early warning symptoms of HA and the importance of accessing rapid emergency care among Bahraini adults attending primary healthcare centers (PHC). The current topic was selected as early treatment of acute coronary syndrome can decrease related mortality and this is the first study of this kind in Bahrain, according to our literature review.
Materials & methods
The observational cross-sectional study included Bahraini adults aged >18 years attending the PHCs during the period of the study. The study was approved, and ethical clearance was provided by the Bahrain Public Health Research Committee. Participants were enrolled in the study from 1st to 5th of May 2016. The inclusion criteria were that the patient had to be a Bahraini origin adult. Exclusion criteria included inability to comprehend Arabic or English, emergency patients or incoherent. Verbal consent was taken from the participants, and educational leaflets were distributed after the interview in order to correct their knowledge about the symptoms of heart attack and the first action to be performed. Confidentiality of participants was maintained.
Data collection and sample size calculation
The Kingdom of Bahrain has 28 health centers distributed into 5 health regions; in this study one health center was selected randomly from each health region.8 Every third person entering the PHC who was fitting the inclusion criteria was invited to participate in the study. The sample population was similar to the overall Bahraini population, as our results were generalizing only to Bahrainis. A standardized interview-based questionnaire was conducted by the family physicians. A leaflet with the five HA symptoms was distributed following the questionnaire to increase awareness during the process.
An optimal sample size was calculated through a sample size table, which included population size, specific margin of error, and a desired confidence level.9 In this study, we considered the population of Bahrain as 1.5 million; confidence level was 95% and a margin of error of 5%. Based on these parameters, the sample size of 384 was obtained, which was approximated to 400 for convenience. Sample of 80 participants were randomly selected from each PHC.9
Standardized questionnaire
We adapted a validated questionnaire from the Behavioral Risk Factor Surveillance System (BRFSS, 2005),10 which was provided by the Center for Disease Control and Prevention. The questionnaire had two parts: demographic data and HA signs and symptoms.10 The demographic data included gender, age, living status, level of education, marital status, and employment; close-ended questions were used. Respondents were asked to identify the five major warning signs and symptoms of HA, which are discomfort of the jaw, feeling weak, chest pain, shoulder pain, and shortness of breath. One question about incorrect sign (decoy question) was asked, which was about sudden trouble with seeing in one or both eyes. Response answers for all questions were "yes," "no," "don't know/not sure”, and "refuse to answer''. We also assessed participants’ knowledge regarding their response to a witnessed heart attack by calling 999. The HA knowledge score was calculated; participants received 1 point for each correct answer. The HA level of knowledge score was out of 7; and the scores were categorized as poor 0–4 and good 5–7 scores points.11
Statistical analysis
The data were entered and analyzed using SPSS 23. The relation between level of awareness and other factors, such as demographic data, health status, and source of medical information were examined using tests of association. Frequencies and percentages were computed for demographic variables, health status variables, source of medical information, and knowledge assessment. Overall knowledge score was computed for the participants. Cross tabulations were performed between knowledge level and each of demographical data, health status data, and source of medical information data. Chi square test was used to determine association between two categorical variables. P < 0.05 was statistically considered statistically significant.
Results
Demographic characteristics of the participants
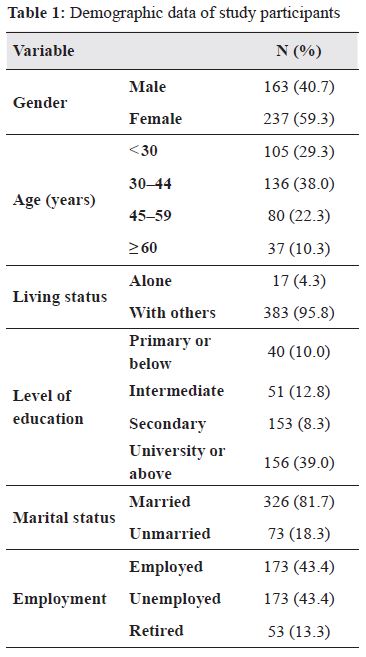
Of the 400 Bahraini participants, a female preponderance (59.3%) was observed. The demographic data of the study participants are described in Table 1. Among the participants, majority (61%) were secondary school graduates or below and 39% had university or above level of education. In addition, 81.7% were married, 95% were living with others, and 43.4% were employed (Table 1).
Knowledge of heart attack symptoms
According to the knowledge score of participants regarding HA symptoms, 71.9% and 28.1% scored poor and good level of knowledge.
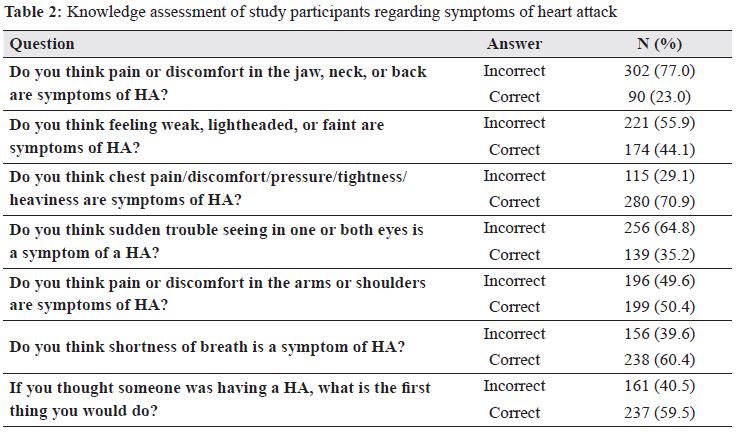
In the study, 70.9% and 60% participants recognized chest pain and shortness of breath as symptoms of HA. Almost, 50.4% respondents correctly recognized that pain in the arms and lightheadedness are symptoms of HA. However, the least identified symptom was discomfort in the jaw, neck, or back.10 Blurred vision, as a symptom of HA, was incorrectly answered by 64.8% respondents. In response to the question about the first action to be performed, while witnessing a HA, 59.5% respondents reported that they would call emergency services (Table 2).
One percent of the participants knew the five correct symptoms of HA, and correctly recognized the decoy symptom and the need to call 999.
Factors associated with knowledge of symptoms
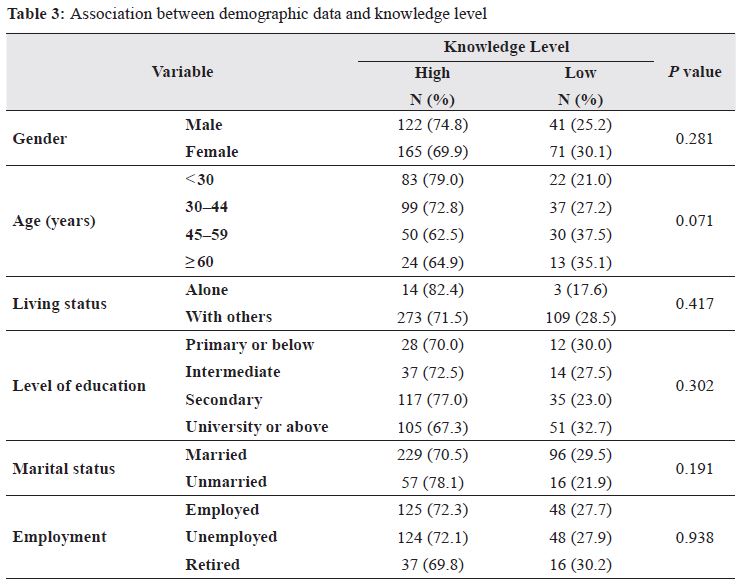
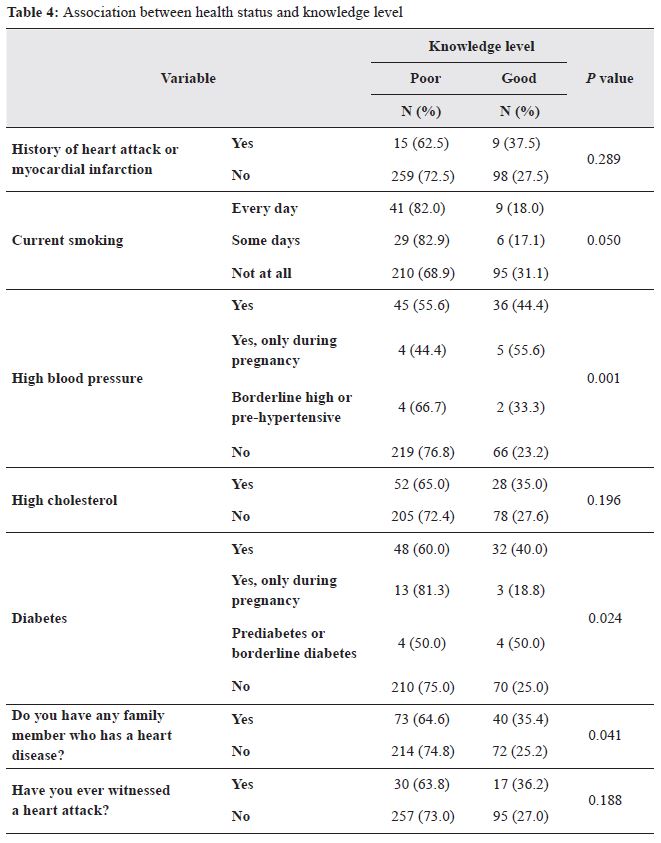
Females had higher knowledge scores as compared to the males (30.1% vs. 25.2%; P = 0.28). Participants with university degree and higher level of education had the highest knowledge score as compared to those with lower level of education (P = 0.302; Table 3). As represented in Table 4, participants with hypertension (44% vs. 23.3%; P = 0.001), highlevels of cholesterol (35% vs. 27.6%; 0.196), anddiabetes (40% vs. 25%; P = 0,024) had betterlevel of knowledge as compared to those withoutthese comorbidities, respectively. On the otherhand, participants who had the habit of smoking hadworse level of knowledge when compared to theircounterparts (18% vs. 31%; 0.05).
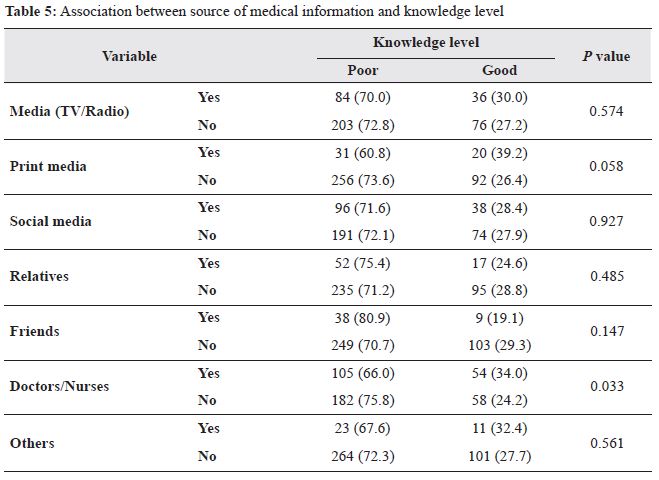
Participants were asked to select a single answerregarding the major source of their medicalinformation. As shown in Table 5, participants whochose doctors or nurses as their major source ofmedical information had higher level of knowledge compared to those who did not (34% vs. 24%;0.033). Respondents who selected social mediaas their source of medical information had betterknowledge score compared to participants who didnot (28.4% vs. 27.94%; 0.927).
The present study revealed alarming results regarding the current level of knowledge of symptoms of HA among Bahraini adults. Only one percent of the participants knew the five correct symptoms of HA, correctly recognized the decoy symptom, and were aware of the need to call 999. The revelation is consistent with the awareness level related to heart disease in all Emirati women in United Arab Emirates (UAE), which was low.12 However, those levels of awareness are considered low as compared to adults in United States of America (10.7%).7
According to our study, females had higher knowledge scores as compared to males. These results were similar to the population of Dubai and Northern Emirates in UAE.13 Further, it was observed that majority of our respondents recognized chest pain as a symptom of heart attack, while other symptoms were less recognized. These findings were similar to the study conducted in UAE.13
Two thirds of Bahraini adults had poor knowledge about HA symptoms and this contrasted with the findings of a Turkish study wherein 23% of the Turkish participants were not aware of the HA symptoms.14
The major sources of medical information among Bahraini adults were doctors/nurses, social media, and television. However, the major sources of medical information among Emirati women were internet (67.2%) followed by friends/relatives (49.3%) and TV (36.1%).12
We observed that participants with hypertension and diabetes had higher level of knowledge as compared to those who did not. We speculate that this might be correlated to the educational role provided by the noncommunicable disease (NCD) clinics in the PHCs in Bahrain.
Consistent with the findings of a German study,15 we observed that patients with a family history of cardiovascular disease risk factors had higher awareness scores. The study suggested that, such patients may be more concerned or anxious about their health.
In our study, we discovered that 60% of the participants would call emergency number in response to HA, in comparison to 32.8% Emirati women from Dubai and Abu Dhabi who would do the same.12 Further, the figures obtained from Gulf Cooperation Council (GCC) were low as compared to United States of America (86%).7 This could be due to the lack of educational campaign about the awareness of HA symptoms and the advertisements regarding such campaigns in the Kingdom of Bahrain and the GCC.
In conclusion, the level of public awareness about HA symptoms in Bahrain is poor. Community health education campaigns are required to increase public health education regarding HA symptoms. It is a responsibility of Public Health Department, Ministry of Health in Bahrain in collaboration with the Cardiac Centre. These campaigns may influence future management of these diseases and improve survival. To our knowledge, this is the first study to address awareness of HA symptoms in Bahrain and in the Gulf Region, offering a platform for further studies.
The authors of the study have no conflict of interest to declare.
We would like to acknowledge the much-appreciated contribution of Dr. Wafa AlSharbti and Family Physician Residency Program in the Kingdom of Bahrain. We genuinely appreciate the efforts of people who agreed to be a part in the research.