
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2020, Volume 32, Issue 3, Pages 9-17
https://doi.org/10.26715/jbms.32_2020_3_2Adel Salman Al-Sayyad1, Fatema M. Alshehabi2*, Duha H. Alabd2, Aalaa A. Marzooq2
1Associate Professor of Family & Community Medicine, Arabian Gulf University, Bahrain.
2General Physician, Ministry of Health, 704, Muharraq, Bahrain.
*Corresponding author:
Dr. Fatema M Alshehabi, General Physician, Ministry of Health, 704, Muharraq, Bahrain; Email: Fatema.M.Alshehabi@gmail.com
Received date: February 04, 2020; Accepted date: August 28, 2020; Published date: September 30, 2020

Background: Medications are the primary tool used to prevent and manage non-communicable diseases (NCD). The medical literature is rich with studies related to the adherence issues of NCD patients to their medication regimen; however, there is a dearth of such studies on patients in Bahrain. Hence, this study was conducted to measure medication adherence among patients with NCD in Bahrain primary health centers (PHC).
Methods: A cross-sectional study was conducted on 400 patients with NCD who were following at PHC in either NCD department or general outpatient clinics between February and March 2019. The data was collected through face-to-face interviews and a questionnaire based on the Medication Adherence Rating Scale (MARS) to measure patient’s adherence to medications.
Results: Only 19.5% of the study participants were adherent. Use of medication reminders was associated with adherence; 49.8% of the participants were not using any reminding method, and 32.3% linked medication timing with their daily activities. Patients diagnosed with more than one disease and married patients were more adherent. There was no statistically significant association between the patients' demographic characteristics and adherence. Following a healthy diet and lifestyle was associated with adherence.
Conclusion: The low level of adherence in patients with NCD indicates the need for increasing awareness, especially regarding the health complications resulting from non-adherence to medications. Doctors must ensure that their patients are adherent to their medication and healthy lifestyles, before making changes in the dosage or medication.
Keywords: Adherence; Bahrain; Chronic disease; Medication; Primary health
Chronic disease is a widely used term and has variable definitions. According to the World Health Organization (WHO), “chronic diseases should have one or more of the following characteristics: they are permanent, leave residual disability, are caused by non-reversible pathological alteration, require special training of1the patient for rehabilitation, or may be expected to require a long period of supervision, observation, or care”.1 On the other hand, the Center for Disease Control and Prevention (CDC) defines chronic disease as “a condition that lasts one year or more and requires ongoing medical attention or a change in lifestyle or both, such as Alzheimer’s disease, arthritis, breast cancer, cervical cancer, colorectal (colon) cancer, diabetes, epilepsy, gynecologic cancer, heart disease, high blood pressure, lupus, multiple chronic conditions, obesity, prediabetes, skin cancer, stroke, tooth decay, and type 2 diabetes.”2
The occurrence of chronic diseases is progressively increasing, resulting in an urgent need for action in health care, especially because of their social and economic impact on the patients’ quality of life. Chronic diseases are caused by multiple factors including genetic, physiological, environmental, and behavioral.3
The term non-communicable disease (NCD) is used to differentiate this group of diseases from communicable (infectious) diseases like hepatitis, human immunodeficiency virus (HIV), acquired immunodeficiency syndrome (AIDS) and tuberculosis.1,4,5 The four major NCDs according to WHO are cardiovascular diseases like heart attacks and stroke, cancers, chronic respiratory diseases such as chronic obstructive pulmonary disease and asthma, as well as diabetes.3
In 2016, NCDs were the cause of 71% of deaths (41 million of 57 million deaths) worldwide. Around 15 million of those deaths were premature deaths (patients’ age 30 to 70 years). There was a significant relationship between premature mortality from NCDs and a country’s economic status. The proportion is extremely high in low- and middle- income countries, where 78% of all NCD-related deaths and 85% of premature deaths occurred.6
Medications are very important for preventing and effectively managing chronic diseases; however, literature-based evidence suggests that a lot of patients with NCDs have problems adhering to their prescribed medication regimen.7 In fact, only around half of them take their medications as prescribed by their doctors.8 According to WHO, adherence to long-term therapies in developed countries is about 50% and is significantly lower in developing countries due to lack of resources and access to health care.1 WHO defines adherence as “the extent to which a person’s behavior – taking medication, following a diet, and/or executing lifestyle changes, corresponds with recommendations from a health care provider.” It suggests that increasing adherence may greatly improve health than any changes in specific medical treatments.1 Non-adherence to medication is estimated to result in 125,000 deaths in the United States (US), mainly due to cardiovascular disease each year.8,9 Furthermore, it is thought that countless doctor visits and admissions, diagnostic tests, and additional treatments could be avoided if patients took their medication as prescribed. Therefore, not only will non-adherence to medication end in a poor clinical outcome, but it will also increase medical expenses and worsen the standard of life.8,9
There are multiple causes of non-adherence to medications such as forgetting to take them, not understanding the instructions. or experiencing side effects. Sometimes it is because of the medication taste, smell, or inconvenient restraints while using the medication (e.g., require avoiding sunlight or milk products). Having to take the medication very frequently or follow complicated instructions makes it hard for some patients to adhere to the regimen. On the other hand, patients can be in a denial phase and not caring about getting better or thinking that the medication cannot help or is not needed. Also, after successfully controlling the disease, they assume that the disease has been sufficiently treated, and they no longer need medication. Other factors that may lead to medication non-adherence include fearing dependence on the medication, encountering obstacles (difficulty swallowing tablets or inability to access the medication), or lack of trust in the doctor.8
In a study conducted on the general population in the US, adherence to medications was found to be 42%. This low level of adherence was related to younger age, ethnicity, using multiple health care providers, and barriers to regular primary care access.9 In India, the adherence to diabetic medications was low at 45.4%, which was associated with the literacy level, duration of the disease, number of chronic conditions, lack of satisfaction in the doctor–patient relationship, treatment at a private facility, and lack of knowledge about the disease and the effect of missing doses.4 In Italy, only 39.3% of the patients were adherent to their medications and those with higher level of education and lesser number of pills per day were more likely to adhere to their medications.5 In the United Arab Emirates (UAE), non-adherence was reported to be as high as 83.3%, which was associated with increase in age, family history of chronic diseases, forgetfulness, and polypharmacy. On the other hand, patients with complications related to a chronic disease were more adherent to their medications.10 In Brazil, non-adherence was reported to be 66.2%; it was higher in men and younger patients.11 In China, 34.9% of the patients showed poor adherence and were mostly in the younger age group, used antihypertensive agents for a shorter duration, employed, and reported their self-perceived health status as being “poor or very poor.”12
In Bahrain, NCDs were the leading cause of death as they accounted for 75% of total deaths in 2017. According to the Ministry of Health Statistics of Bahrain, 67.75% of the population had been diagnosed with at least one of the NCDs.13 There is scarce literature on adherence to medications by NCD patients. Therefore, so we conducted this study to measure medication adherence among patients with chronic diseases in primary health care in Bahrain.
A cross-sectional study was conducted on patients with chronic diseases who were followed up at primary health centers (PHC) in both general outpatient clinics and NCD clinics in February and March 2019. A multistage sampling strategy was used to select a total of 400 patients. There were a total of 28 health centers distributed within the four governorates of Bahrain; the Capital, Muharraq, Northern, and Southern. A total of eight health centers (two from each of the four governorates) were selected and 50 patients were recruited from each health center. Within each health center, NCD patients were seen either in the general or in the specialized NCD clinics. The researchers randomly recruited 50% of the patients seen in the general clinics and the other 50% from the NCD clinic. The research team approached all eligible patients from the NCD and general clinics attending each of the selected health centers during the study period for their appointments. Patients were eligible only if they were aged ≥18 years, had been diagnosed with at least one chronic disease, and had an active prescription without change for at least 90 days. Patients with cognitive impairment and psychiatric diseases were excluded. The selected participants were screened for eligibility and those eligible were recruited after obtaining their consent, until the designated sample size was reached.
The sample size was estimated based on the following: the number of people diagnosed with a chronic disease, a 95% confidence interval (CI), a 5% tolerated error, and a design effect of 2. With an allowance of 10% for non-response, the final sample size was calculated to be approximately 400 patients.14
Face-to-face interviews were conducted by the researchers in the waiting area of the health centers. The patients were informed about the study objectives and the importance of their participation and were allowed to ask any question. Also, they were informed that their participation was voluntary and that they could withdraw from the interview at any time. They were assured that their responses would be treated in confidence and complete anonymity was maintained. Patients did not receive any incentive for their participation.
The interview addressed six primary themes:
(i) basic information (age, gender, marital status, number of children, the highest level of education, employment status, and economic status);
(ii) healthy lifestyle;
(iii) medical history (chronic diseases diagnosed with name, number, and length of medication use; and family history of chronic disease);
(iv) patient’s main source of information about his medical condition or therapies prescribed;
(v) use of medication reminders; and
(vi) adherence to prescribed medications.
The Medication Adherence Rating Scale (MARS) was used to measure the patients’ adherence to medications over the four weeks preceding their medical specialist’s visit. This scale measures adherence with the help of 10 questions that require yes/no responses, as shown in Table 1.
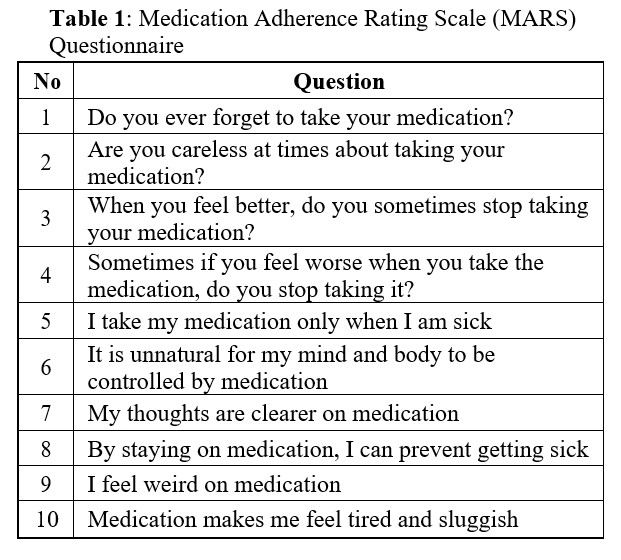
The first six questions (Q1-6), Q9, and Q10 are scored “No = 1” and “Yes = 0,” while Q7 and Q8 are scored as “No = 0” and “Yes = 1”. The total score will then reflect the degree of compliance – compliant if the score is high and non-compliant if it is low. Patients are compliant if they respond “No” to Q1-6, Q9, and Q10 and “Yes” to Q7 and Q8. A score of 10 is considered adherent and less than 10 indicates non-adherence. 15
The number of medications was recorded for each participant. It was divided into polypharmacy (the use of 5 or more medicines) or non-polypharmacy (use of 4 or less medications).16
The demographic and lifestyle characteristics of the 400 study participants are presented in Table 2. The age range was 30-90 years, and about half (51%) of them were 30-60 years old. The majority were female (57.8%), and most of them were Bahrainis (89.8%). The vast majority (87.30%) of the patients were married, 18% of them were illiterate, and about half of them (52.6%) had at least a high school degree or more. More than one-third (37%) were housewives, and 29% were working. Most of the patients (82.5%) considered their economic status as medium, and only 4.8% had a high income. Regarding the lifestyle of the study participants, only 8.8% of them were smokers and around 32.20% of them were exercising for at least 20-30 min/day for 3-5 days/week. More than half (58.8%) of the patients reported having 1-2 servings of fruits and vegetables per day, while only 5.8% patients were eating more than five servings/day, and 12.30% reported not eating fruits or vegetables at all (Table 2).
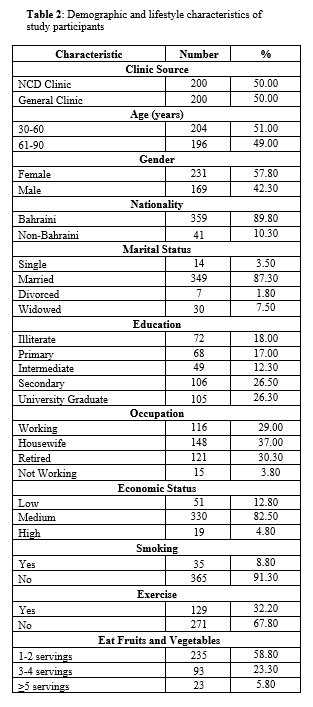
Table 3 shows the prevalence of chronic diseases and the use of medications by study participants.
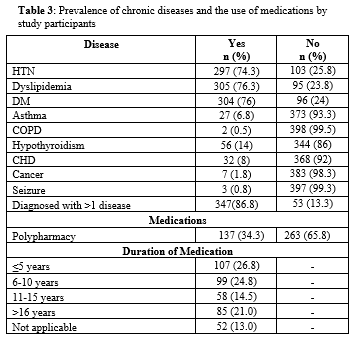
The majority (86.8%) of the study population was diagnosed with more than one disease while 13.3% had only one disease. Around 74.3% were diagnosed with hypertension, 76.3% with dyslipidemia, 76% with diabetes, 6.8% with asthma, 0.5% with chronic obstructive pulmonary disease (COPD), 14% with hypothyroidism, 8% with CHD, 1.8% with cancer, and 0.8% with seizure.
Around one-third (34.3%) of the study participants were using more than five medications. The duration of the medication use varied: 26.8% had been using for ≤5 years, 24.8% for 6-10 years, 14.5% for 11-15 years, and 21% for ≥16 years (Table 3).
Around half (49.8%) of the study participants were not using any reminding method for taking the medication. Of the remaining half who reported using medication reminders, 32.3% were linking medication timing with their daily activity, 7.2% were using a pill organizer, and 6% were depending on family or friends to remind them to take the medication (Figure 1).
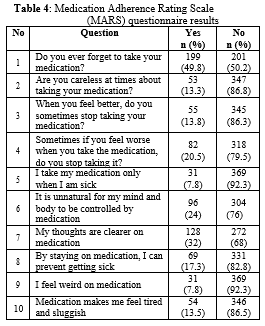
Table 4 shows the detailed responses of participants to the MARS questionnaire. Almost half (49.8%) of the participants reported that they occasionally forget to take their medicines, 68% did not feel stable or had unclear thoughts about medications, 82% did not believe that medicines could prevent the disease from getting worse.
The questionnaire revealed that only 19.5% of the study participants were adherent (Figure 2).
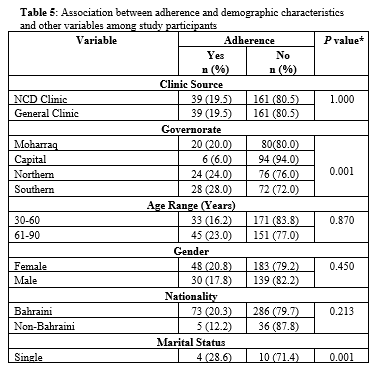
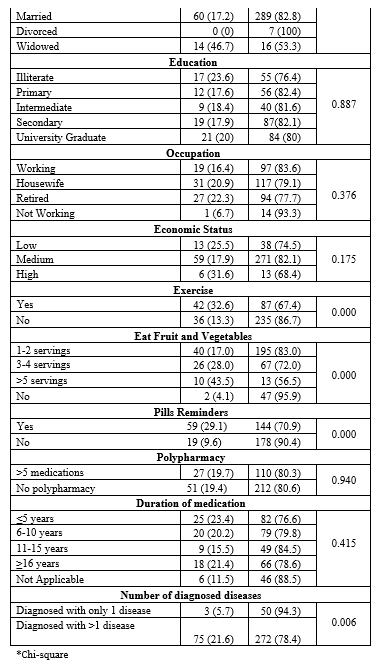
Table 5 demonstrates the association between adherence and demographic characteristics and other variables among study participants. There was no statistically significant difference in the adherence rate between patients recruited from NCD clinics or general clinics (Pvalue 0.207). On the other hand, married patients appeared to be more adherent in comparison to single, divorced, and widowed patients (P=0.001). There was no statistically significant association between age, gender, nationality, education level, occupation, or economic status with adherence. Following a healthy diet and lifestyle was significantly associated with adherence – patients who reported exercising for at least 20-30 min/day for 3-5 days/week were more adherent (P=0.000), patients who ate fruits and vegetables were more adherent than those who did not (P=0). Using reminders was significantly associated with adherence (P=0.000). Patients who were diagnosed with more than one disease were more adherent (P=0.006). Polypharmacy (>5 medications) and duration of medication use were not associated with adherence (P=0.940 and 0.415, respectively).
This study is the first in Bahrain to measure medication adherence among patients diagnosed with chronic diseases attending primary health care centers in Bahrain. It revealed that the adherence rate was low (19.5%) among the study participants.
The adherence rate found in this study is similar to that reported in the UAE, which had 16.7% adherence to chronic disease medications.10 On the contrary, this rate is lower than that reported from other countries like the United States of America with 28.6% adherence among the general population, India had 54.6% adherence in diabetic patients, Italy had 39.3% among patients with chronic disease, Brazil showed 33.8% adherence among epileptic patients, and 65.1% of Chinese patients receiving antihypertensive medication were considered adherent.4,5,9,11,12
There was a belief that patients who were visiting the NCD clinic were more likely to be adherent than those visiting the general clinic at health care centers, but this study showed that the adherence rate was the same in both clinics, which could be because there is no particular program to encourage patients’ adherence in both clinics.
In contrast to other studies, several variables were found to have no association with adherence. Both genders had an almost equal rate of adherence.11 Occupational and economic status were not associated with adherence, which is likely due to the accessibility of free health care services in Bahrain.12 Correlation of adherence with the educational status could be due to the increase in awareness and known health complications of chronic disease in patients.4,5
Age groups were divided into two categories, as explained earlier. In contrast to other studies, age appeared to have no significant correlation with adherence.9-12 It is worth mentioning that most of the participants were in the older age range. Therefore, the adherence level in young patients with chronic diseases might not be well represented in this study although some studies suggest lower adherence levels in younger patients due to immaturity and lack of background information about chronic diseases, in comparison to older age groups.9
Medication adherence can be affected by many factors such as patients who exercised, ate fruits and vegetables - especially those who ate ≥5 servings per day - were more adherent, which is a factor that was not studied before. These patients who maintain a healthy lifestyle seem to know its impact not only on their chronic disease but also on their overall health. Also, the adherence among patients diagnosed with more than one disease was higher in contrary to other studies, and this could be due to patients’ awareness of non-adherence complications as already experienced by them.4
Furthermore, polypharmacy was not associated with adherence, which is inconsistent with other studies and this most likely was because patients overcame this obstacle by using medication reminding methods such as linking it with daily activities.5,10 The patients who were using reminding methods were more adherent than those who were not.5 In fact, this could be the reason why 49.8% of the patients forgot to take their medicines.6,10 The duration of medications taken was also not a risk factor, which is inconsistent with other studies.12
It is worth mentioning that the use of adherence-measuring tools such as MARS used in this study has some limitations1 as some patients might provide socially acceptable answers, which in turn lowers the accuracy of the data. Moreover, comparison of adherence rate between different countries and settings should be considered with caution due to the variability in population and cultural differences, data characteristics and collection, adherence-measuring tools, the diversity in the health care system such as primary or secondary health care, cost, and accessibility around the world.
The level of adherence in patients with chronic diseases, attending primary health care centers, was low (19.5%). This finding suggests that there is a need for more awareness among patients, especially regarding the complications and health consequences of non-adherence to their medication. Also, instead of increasing the dose or changing medications, doctors must make sure that the patients adhere to their medication regimen and follow healthy lifestyles.