
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2020, Volume 32, Issue 3, Pages 23-25
https://doi.org/10.26715/jbms.32_2020_3_9Mahmood Al Amm1*, Fatima Fatima Naser Abdulaziz2
1Corresponding author, Orthopedics resident, Salmaniya Medical complex, Bahrain.
2Co-author, Orthopedics consultant, Salmaniya Medical complex, Bahrain.
*Corresponding author:
Mahmood Al Amm,Orthopedics resident in Salmaniya Medical complex, Bahrain; Email: ma.ajalel@gmail.com
Received date: May 26, 2020; Accepted date: July 26, 2020; Published date: September 30, 2020

Neglected developmental hip dysplasia can present with many complications, this case report presents a case where a bony prominence on the femoral neck occupied the acetabulum and functioned as a femoral head. This case report discusses the clinical and surgical approach to this unique presentation of a neglected case of developmental hip dysplasia and briefly reviews the relevant literature which reports few similar cases.
Keywords: Braces; Hip dislocation; congenital/diagnosis; Hip dislocation; congenital/therapy; surgery; complications; Infant; Orthopedics procedures
Neglected developmental hip dysplasia (DDH) presents late with a variety of symptoms that are often the result of chronic changes to the acetabulum and the articular surface of the bone that is working as joint surface. While delayed diagnosis of developmental hip dysplasia and lack of patient compliance are usually the reasons of a neglected hip dislocation, this case presents a patient who underwent closed reduction that failed with a subsequent loss to follow up despite obvious symptoms and then a late presentation with the sequelae of neglected DDH. A closed reduction approach of dislocated hips in developmental hip dysplasia is associated with multiple complications that include the risk of failed reduction, avascular necrosis of the femoral head or femoral nerve impingement.1 Some of those complications can be reduced with ensuring a concentric reduction without excessive flexion or excessive abduction. In 12%-43% of cases a closed reduction attempt fails to produce a stable concentric reduction of the hip.2 This encourages early detection with a closed reduction approach which has its best chance while in the first 6 months of life or early operative repair as a mean of ensuring satisfactory reduction and avoiding a late operative intervention which may be less effective and carries a higher risk of long term limitation in the range of motion as bones are less likely to remodel with age.3 Achieving early stable reduction of the dislocation is hence the key to avoiding the complications that occur with long term changes that affect a chronically dislocated hip.4
Few reports in the literature describe the greater trochanter serving as a false femoral head, with an atrophic femoral head that is displaced from the acetabulum.5 This case presents a bony prominence on the neck of the femur serving as the articular surface with the acetabulum, with a deformed femoral head due to chronic neglected developmental hip dysplasia.
A 2-year-old female child presented to the orthopedics clinic complaining of left hip discomfort, limping, and limitation of movement that started after the removal of the hip Spica that she was placed in. The patient’s care taker reports that the child was diagnosed with developmental hip dysplasia at the age of 1 year, and underwent a closed reduction followed by immobilization with a hip Spica in flexion and abduction at another medical center; after which she was lost to follow-up despite experiencing symptoms of dislocation such as limping and limitation of movement until her current presentation. The caretaker denied any history of trauma or recent falls after the closed reduction attempt. On examination no apparent joint deformity or tenderness was noted, however a clear leg length discrepancy was noted. Range of motion showed limited abduction with no other limitations and neurovascular status was intact with no deficits.
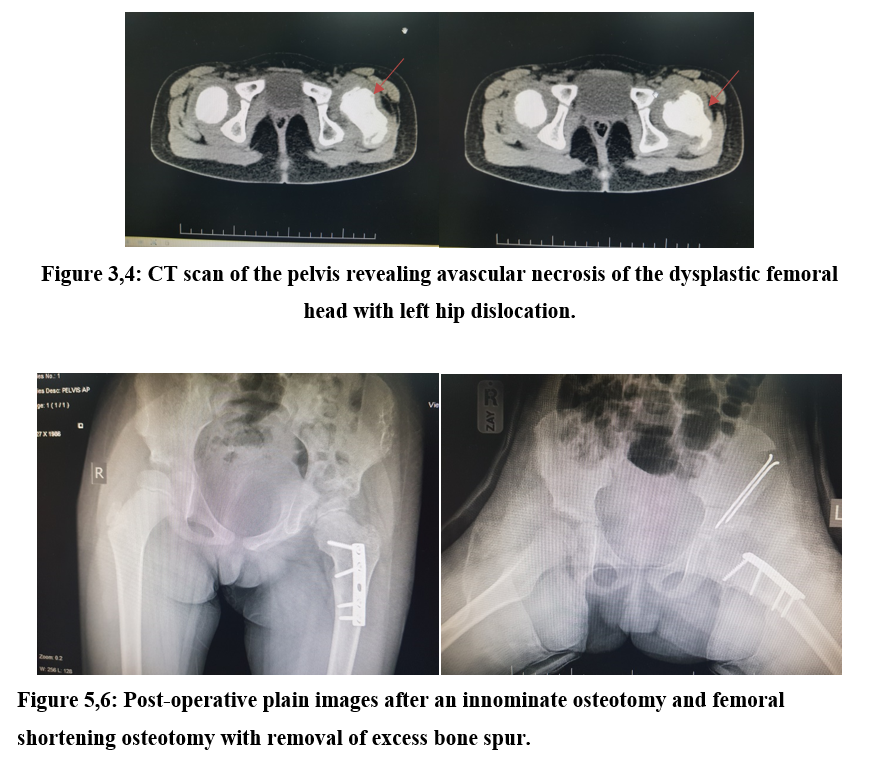
Multiple radiographs were taken of which two images are presented in Figure 1,2 that showed clear dislocation of the left hip with a deformed ipsilateral femoral head, a bony prominence located on the inferior aspect of the femoral neck occupied the acetabulum as a false femoral head. A CT scan was done (Figure 3,4) which revealed elements of avascular necrosis of the femoral head with the femoral neck directly opposed to the acetabulum. Open reduction was then recommended. The anterolateral approach to the hip was adopted, the acetabulum was approached in the plane between sartorius and vastus lateralis until the hip joint capsule is reached. A T-shaped incision was made over the hip joint capsule, the femoral head and round ligament were identified, the ligament was transected to reveal a hard-bony structure occupying the acetabulum. Intraoperative radiographs confirmed the previous findings, and a cartilaginous covering was found overlying the bony prominence that was found occupying the acetabulum. The femoral head was reduced back into the acetabulum after transecting the transverse ligament of the acetabulum and mobilizing the iliopsoas muscle. A Salter osteotomy of the iliac bone with fixation using a Kirshner wire and femoral varus de-rotation shortening osteotomy with fixation of the bone with plates and screws were done. The bony prominence was removed, and the hip reduced in attempt to restore normal morphology of the hip, radiographs were taken intraoperatively to confirm satisfactory reduction and restoration of hip morphology (Figure 5,6).
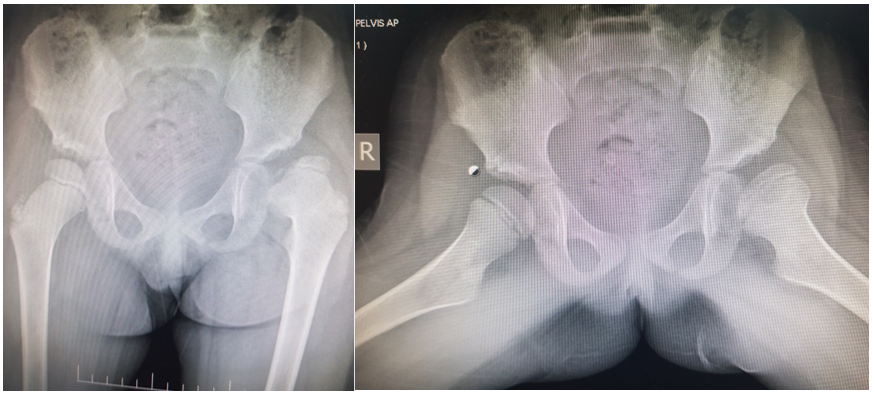
Figures 1,2: Pre-operative plain radiographs of the hip joints showing left hip dislocation with femoral head dysplasia
Post operatively the patient was placed in a hip spica for 6 weeks, after which the spica was removed and joint was examined, with removal of the K-Wire. She was then re-placed in a hip spica cast. The cast was removed after another 6 weeks and the patient underwent close follow-up with multiple physiotherapy sessions. The patient was evaluated postoperatively using the McKay clinical criteria which showed a good rating, with a grade II recovery.6 She experienced a significant improvement in her symptoms with complete resolution of the pain and limping and improvement in the leg length discrepancy with a mild residual limitation of abduction of the affected hip. The patient was followed post-surgery for 1-year duration with multiple visits at various intervals starting from weekly to monthly to bi-monthly on an outpatient basis. The patient is still being followed with regular appointments with the orthopedics outpatient clinic.
This case reports a rare presentation of neglected developmental hip dysplasia that resulted from a closed reduction attempt that failed and reverted into dislocation after stabilization with a hip Spica. This resulted in a bony prominence taking over the function of the femoral head and functioning as the articular surface with the acetabulum. With resultant avascular necrosis of the dislocated femoral head.1 This highlights the value of early recognition and reduction of developmental hip dysplasia, and the value of early reduction to achieve satisfactory and stable opposition of the femoral head with the acetabulum to avoid late surgical intervention which may carry higher rates of complications. Closed reduction remains a very effective modality of treatment for developmental hip dysplasia; the choice between closed or open methods of reduction is then better decided on an individual case by case basis. This case for example has failed attempts of closed reduction, was ambulatory and presented late at the age of 2, which made operative intervention the only method for satisfactory recovery of her hip dysplasia.
It is imperative to closely follow-up such patients should a closed reduction be chosen as the appropriate course of management even with appropriate stabilization with a spica cast and ensuring proper concentric reduction of the dislocated hip. Early detection of the dislocation especially before 18 months of age carries a better chance of success as remodeling is fast and slows down with age, and post reduction follow up to detect complications is also key to avoiding surgical intervention and achieving a stable closed reduction result.
Authors are employed by the ministry of health and have no other affiliations. No funding or sponsorship were received from any entity and there is no notable conflict of interest to declare.