
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2020, Volume 32, Issue 3, Pages 30-33
https://doi.org/10.26715/jbms.32_2020_3_5Hussam Hassan Ismail1*, Mohamed A. Tawab2, Abdulmenem Yahya Abualsel3, Alaa A. Ayad4, Tamer Fathi Ali5
1Department of Radiology, Radiology Registrar, MBBS, MSc, FEBR, ABR, King Hamad University Hospital, Bahrain
2Department of Radio-diagnosis, Consultant radiodiagnosis, MBBS, MSc, MD, King Hamad University Hospital Bahrain
3Department of General Surgery, Consultant and Head of Surgery Department, MBBS, MSc, MD, King Hamad University Hospital, Bahrain
4Department of Radiology, Senior Registrar, MSc, MD, FRCR, King Hamad University Hospital, Bahrain
5Department of Radiology, MD, Faculty of Medicine, Zagazig University, Egypt
*Corresponding author:
Dr. Hussam Hassan Ismail, Department of Radiology, Radiology Registrar MBBS, MSc, FEBR, ABR, King Hamad University Hospital, Bahrain. Email: drhusam19@gmail.com
Received date: May 14, 2020; Accepted date: August 10, 2020; Published date: September 30, 2020

Cecal volvulus describes the rotation of a mobile cecum around its mesentery which frequently leads to large intestine obstruction. Anatomically, this can occur in a meso-axial or an organo-axial pattern. Thus, Cecal volvulus has a wide range of presentations which can vary from mild intermittent to severe acute abdominal pain. However, if not treated in a timely manner, it can result in high morbidity due to sepsis and intestinal strangulation.
Cecal volvulus predominantly affects female patients aged between 40–60 years specifically those with a history of chronic constipation. Incomplete intestinal rotation during fetal life also plays an important embryological factor in cecal volvulus development.
In this case report, a 30-year-old female presented with severe lower abdominal pain continuously occurring for 6 hours. A previous history of constipation and minimal bowel movement was noted.
The purpose of this report is to highlight imaging findings needed for diagnosis and management of this rare serious condition.
Keywords: Abdominal pain; Cecum; Intestinal obstruction; Intestinal strangulation; Volvulus
Cecal volvulus describes the rotation of a mobile cecum around its mesentery which frequently leads to large intestine obstruction and can occur in a meso-axial or an organo-axial pattern.1
Cecal volvulus is responsible for approximately 1–1.5% of all intestinal obstructions and its annual global incidence is estimated to be about 2.8 to 7.1 per million of the general population.2 It is attributed to large intestinal obstructions in about 1 to 3% of cases. 3,4 Patients experience a wide range of clinical presentations from mild intermittent to severe acute abdominal pain. However, if not treated in a timely manner, it can lead to sepsis, perforation, peritonitis and intestinal strangulation.5,6
From an embryological point of view, the anatomy of the cecal and pericecal peritoneum has a late determination (5th gestational week). During the final period of intestinal embryogenesis, the caecum rotates counterclockwise from the left abdominal position to its final right lower abdomen position with simultaneous fixation of the right colon mesentery to retroperitoneal structures.7,8 Incomplete intestinal rotation can result in insufficient fixation of the right colon predisposing to cecal volvulus.
Other contributing factors such as prior abdominal surgery with postoperative adhesions were noted in about 53% of cecal volvulus cases (that can act as fixation points and the fulcrum of rotation for the right colon), late term pregnancy, high fiber intake and history of chronic constipation. 5,9,10, 11-13
A 30-year-old female presented to the Emergency Department with severe lower abdominal pain lasting for 6 hours associated with a few episodes of non-bilious vomiting, there was no cessation of flatus or bowel movement. Past medical history included chronic constipation and decreased bowel movement since a year, (history of ≤2 bowel movements per week with hard large stool despite taking laxative granules and hypothyroidism with no previous surgical history. Positive findings on clinical examination included abdominal distension and generalized tenderness with no rebound or guarding. She has never experienced such severe pain before.
CT scan of the abdomen and pelvis showed dilated large bowel and markedly dilated caecum with abnormal position in the mid abdomen. The characteristic "whirl sign" of cecal mesentery was noted which is pathognomonic for cecal volvulus (Figure 1A-D).
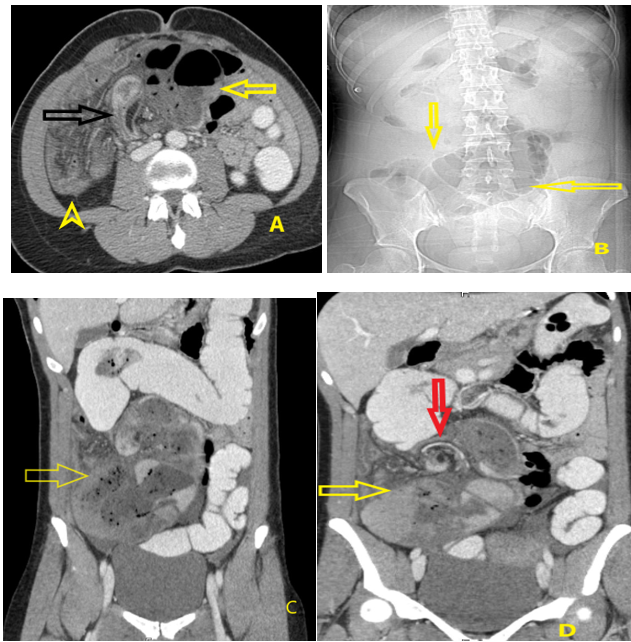
Figure (1): (A) The axial CT scan shows small bowel loops (arrow head yellow) lateral to dilated cecum (yellow arrow) and abrupt transition bird beak sign (black arrow), (B) scout view showing a dilated cecum (yellow arrow),(C) coronal CT showing dilated cecum (yellow arrow), (D) coronal CT showing whirling and swirling of mesenteric vessels ( red arrow) at its transition to a collapsed colon
An emergent exploratory laparotomy (Figure 2) was carried out, which confirmed the diagnosis of cecal volvulus. Therefore, cecal detorsion, and cecopexy was performed by fixing the cecum and a part of ascending colon to the abdominal wall, appendicectomy was done uneventfully. A rectal tube was utilized for deflation of gases. The patient was stable throughout the procedure and was discharged after three days.
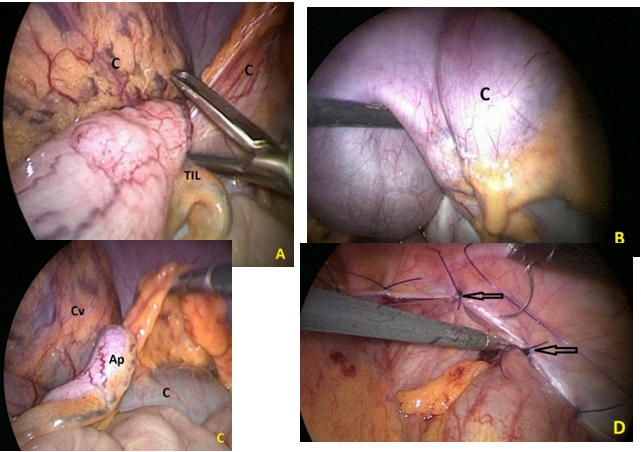
Figure (2). Laparotomy images (a-c) showing cecal volvulus (AP: appendix, TIL: terminal ileum, C: Cecum and Cv: Cecal volvulus) and (d) showing Cecopexy (black arrows)
Cecal volvulus involves axial twisting of the cecum usually in a counterclockwise manner. It is considered an uncommon cause of acute intestinal obstruction.2-4,5,8-10
This is our first case of cecal volvulus case for 8 years.
Our patient’s sole predisposing factor for cecal volvulus development was that she was an adult female. Moreover, the complaint of chronic constipation lasted for more than 1 year despite taking laxative granules and she had also a mobile cecum as well.
Cecal volvulus has a wide range of presentations which can be mild intermittent to severe acute abdominal pain due to intestinal strangulation and ischemia that results from mesenteric vascular obstruction by twisting as was presented in our patient.8
The role of laboratory tests is limited as they have no significant diagnostic specificity or sensitivity. Radiography is usually the first line in imaging investigation for cecal volvulus, but CT confirms the diagnosis in 90 % cases.10 It appears as a dilated cecum almost 100% cases, absent distal colonic gases in 82%, while small bowel can be dilated in around 50 %.12,13
The features shown on CT include a midline markedly distended cecum (sometimes known as the Coffee bean sign, more common with sigmoid volvulus type and not demonstrated well in our case), two ends of the bowel converging towards a torsion point (known as the bird beak sign), the mesentery showing a swirling pattern of fat, and congested vessels (known as the whirl sign that occurs when afferent and efferent bowel loops rotate around a fixed point of obstruction, which results in tightly twisted mesentery along the axis of rotation which was a key finding to establish the diagnosis of cecal volvulus in our case at the time of presentation). 10,13,14
A diagnosis of Cecal volvulus requires surgical intervention to reduce the morbidity and mortality of patients. An emergent exploratory laparotomy is usually performed to confirm the diagnosis of cecal volvulus.
In our patient there was no intestinal gangrene, hence Cecal detorsion and cecopexy is only required for the fixation of the cecum to prevent recurrence.15
After 2 and 6 weeks of follow up, the patient is getting better with no recent complaints, no vomiting, no constipation, or loose stools.
This study was approved by Head of Scientific Development and Research at KHUH. as well as informed consent from the patient included in this study was taken.
Consent was obtained from the patient for publication.
The data that support the findings of this study are available on request from the corresponding author.
Not applicable.
Not applicable