
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2020, Volume 32, Issue 3, Pages 34-39
https://doi.org/10.26715/jbms.32_2020_3_6Sufyan Nisar Ahmed Ansari1*, Kanak Ketan Ganguly2
1Sufyan Nisar Ahmed Ansari, Senior Resident, Dental and Maxillofacial Department, Bahrain Defence Force Hospital, Riffa, Kingdom of Bahrain
2Kanak Ketan Ganguly, Chief Resident, Periodontology, Dental and Maxillofacial Department, Bahrain Defence Force Hospital, Riffa, Kingdom of Bahrain.
*Corresponding author:
Dr. Sufyan Nisar Ahmed Ansari, Senior Resident, Dental and Maxillofacial Department, Bahrain Defence Force Hospital, Riffa, Kingdom of Bahrain; Email: Sufyan.ansari@bdfmedical.org; Tel. No.: (+973)-39274704
Received date: July 02, 2020; Accepted date: August 13, 2020; Published date: September 30, 2020

The anterior teeth usually need immediate replacement after extraction to fulfill the esthetic and related psychosocial requirements of the patient. The numerous techniques available to clinicians for this purpose are either expensive, uncomfortable, technique-sensitive, laboratory-intensive, or fragile. This article describes a chairside method of creating an immediate bonded replacement that is tailor-made to the patient’s oral cavity and overcomes most of the limitations mentioned above. The life-like composite resin – ovate pontic – is fabricated at the chairside, rapidly and effortlessly. All the steps and materials used are described in detail to enable any dental clinician to emulate the same when faced with a similar situation. Additionally, the case has been recorded in vivid photographs that are self-explanator.
Keywords: Artificial tooth, Composite resins, Immediate partial denture, Resin-bonded Fixed Partial denture, Temporary dental restoration
Extraction of teeth in the anterior region of the mouth may be required due to dental trauma, carious destruction, or advanced periodontal disease. The inevitable gap resulting from the removal of the anterior tooth is embarrassing for the patients in social and professional life,1 and they often demand immediate restoration of the unesthetic space.2 There are multiple options available at the clinician’s disposal to provide a quick provisional replacement of the resulting space in the form of an immediate denture, resin-bonded bridge, or implant-supported prosthesis to satisfy the patient’s need.3-5 However, these options may require adequate planning, multiple appointments, laboratory support, and may not be suitable where emergency extraction is needed such as in cases of traumatic dental injuries.6,7 Additionally, immediate implant placement may not be feasible in , and certain clinical conditions may require a two-staged implant technique with a provisional restoration for esthetic reasons.7,8
Several other simpler methods and materials have been described in the literature for the immediate replacement of the lost anterior tooth.6 These may utilize a pontic made of acrylic resin, composite resin, or natural tooth crown bonded to the abutment tooth with etch-retained resin composite. Moreover, fiber or wire reinforcements have also been utilized to improve the strength and retention of the pontic at the unprepared abutment tooth site to serve as a long-term provisional replacement of a missing tooth.9
This case report illustrates a simple chairside method of ‘ovate pontic’ fabrication using conventional resin composite for the replacement of an anterior tooth planned for extraction. The procedure proposed here is a slight modification of similar techniques previously described in the literature, tailored to the presenting clinical scenario.10 Furthermore, simultaneous restorative treatment of neighboring anterior teeth has also been described to enable an appreciation of the complete clinical process.
A 25-year-old medically fit male patient presented at an emergency dental clinic of Bahrain Defence Force (BDF) Hospital in April 2019 complaining of a broken tooth, mild pain, and foul smell from the anterior region of the mouth. He also complained about poor appearance due to the fractured tooth and failing discolored restorations in neighboring anterior teeth. He reported that the front tooth was slightly fractured a few months ago, but it had gradually broken down entirely. He remembered having a root filling done in the same tooth more than five years ago and also mentioned that several previous attempts to restore the tooth had failed. He had also noticed a small swelling that appeared to be related to the fractured tooth. Being an irregular dental attendee, he only visited a dentist once a year for scaling or if any emergency dental care was required. His oral hygiene measures included brushing twice daily with a fluoride-containing toothpaste without any interdental cleaning aids. He admitted to being a teetotaler, non-smoker, and denied using tobacco in any form. He did not report any significant stress in life. Dietary analysis of the patient did not reveal any consumption of substantial amount of cariogenic food except tea once a day with 1-2 teaspoons of sugar. However, he admitted to eating chocolates and drinking cold drinks in the past during outdoor activities with friends. He is not aware of clenching or grinding his teeth.
Extraoral examination was unremarkable, whereas intraoral soft tissue examination showed the opening of the sinus on the alveolar mucosa labial to the fractured tooth 12 (Figure 1a). Tooth 12 was fractured to the gingival level, and caries were still evident on the remaining tooth structure. Discolored resin composite restorations were present on teeth 11, 21, and 22 that were imparting a poor overall appearance (Figure 1a). In addition to deep palatal pit caries on tooth 22 (Figure 1b), several other carious teeth were noted in both the quadrants. Periodontal assessment showed generalized moderate periodontal disease with plaque and bleeding scores of 46% and 47%, respectively.
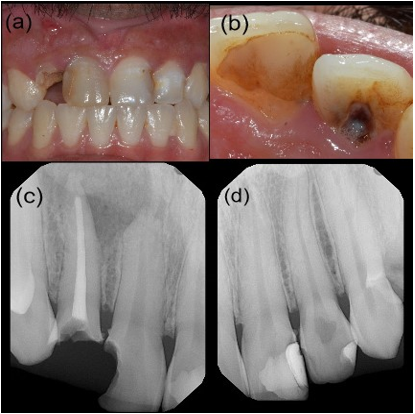
Figure 1 (a-d): Pre-operative view showing fractured tooth 12 with associated sinus and discolored restoration on neighboring teeth (a). Deep pit caries evident on tooth 22 with discolored resin composite restoration on tooth 21 (b). Periapical radiographs of teeth 11, 12, 21, and 22 (c&d).
Cold sensitivity testing was performed on teeth 11,13,21,22, and 23 using Endo-Frost (Roeko, Langenau, Germany). Teeth 13, 21, 22, and 23 reacted positively, whereas tooth 11 showed no response to the cold test. No tenderness to percussion was noted on teeth 11, 12, 21, and 22. Periapical radiographs (Figures 1c and 1d) showed inadequate endodontic treatment of tooth 21 with a large periradicular radiolucency. The previous restoration of tooth 11 was dislodged during the examination to reveal a large cavity near the pulp. Periradicular radiolucency and shortening of the root of tooth 11 could also be seen on the radiograph. Recurrent caries were evident on teeth 21 and 22, but no periradicular changes were noted. The prognosis of tooth 12 seemed poor, whereas teeth 11, 21, and 22 appeared to have a good prognosis if adequate restorative treatment was provided.
The following diagnoses were made based on the clinical and radiographic examination:
The main goal of primary treatment was to educate and motivate the patient to take responsibility for his oral health care. The treatment was aimed at halting the disease process and preventing its progress and restoration of the anterior teeth to a level acceptable to the patient. The treatment plan involved endodontic treatment of tooth 11; restoration of teeth 11, 21, and 22; extraction of tooth 12; and immediate replacement with chairside constructed resin composite pontic bonded to adjacent teeth.
Emergency treatment was initiated with endodontic treatment and pre-endodontic restoration of tooth 11. Local anesthesia (LA) was administered using 2% lidocaine with 1:100000 epinephrine (labial infiltration). The caries were removed and the access cavity prepared using the Endo access kit (Dentsply Sirona, Charlotte, USA). After the root canal orifice was identified, the rubber dam (RD) was placed to isolate tooth 11. A cotton pellet was placed in the pulp chamber space, and the cavity was etched using Vococid 35% orthophosphoric acid (VOCO GmbH, Cuxhaven, Germany). After the application of Adper Single Bond Universal Adhesive (3M, St Paul, USA), resin composite build-up was done using Filtek Z250 XT (3M) universal nanohybrid resin composite shade A2.
Filtek Z250 XT (3M) universal nanohybrid resin composite shade A2 was used to fabricate a pontic using a tooth mold from the Essentia composite kit (GC, America) (Figure 2a). The pontic was trimmed using a high-speed diamond bur to create an ovate shape to fit in the extraction socket to support the soft tissues (Figure 2b). Tooth 12 was extracted atraumatically using a straight elevator and maxillary incisor forceps (Figure 2c). The approximal surfaces of teeth 11 and 13 and pontic were etched, and the adhesive was applied as described above. The pontic was placed in the extraction socket at least 2 mm below the gingival margin and bonded with teeth 11 and 13 (fixed-fixed) using FiltekTM Supreme Ultra Flowable Restorative (3M) and reinforced with Filtek Z250 XT (3M) universal nanohybrid resin composite shade A2 (Figure 2d). The fixed-fixed design was used as tooth 11 lacked enamel for bonding and to provide more rigidity to the bridge. The final finishing and polishing were performed using fine diamonds and Enhance PoGo (Dentsply Sirona) polishing system. A 0.2% chlorhexidine mouthwash Corsodyl (GSK, UK) was prescribed to be used three times a day for a week.
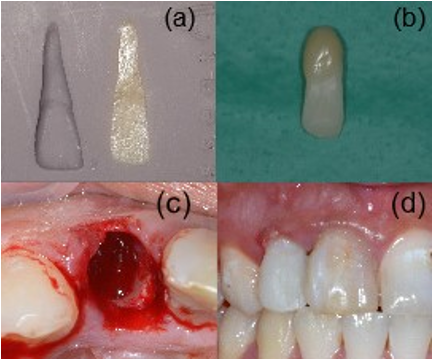
Figure 2 (a-d): Fabrication of resin composite pontic using tooth mold (a&b). View immediately after extraction of tooth 12 (c). Cementation of the pontic with adjacent teeth immediately following extraction (d)
On subsequent visits, restoration of teeth 21 and 22 was completed as shown in Figures (3 a-d). After the completion of the endodontic treatment of tooth 11, the pontic 12 was removed and its tissue surface was adjusted to match the soft tissue profile of the healing extraction socket (Figure 4a). The pontic was then again splinted to the abutment teeth using Filtek Z250 (3M) resin composite shade A2 reinforced with SUPER-SPLINT (Hager & Werken GmbH & Co., Duisburg, Germany) glass fiber tape (Figure 4b). The fiber-reinforced bridge was left in situ as long-term provisional restoration until the oral hygiene was stabilized and the patient decided for a more definitive replacement option. The patient was recalled after 3 and 10 months of final splinting of pontic 12 as shown in Figures 4c&d. Oral hygiene instructions were the mainstay of the treatment phase and were reinforced at every treatment visit with particular emphasis on the use of Oral-B super floss (Procter & Gamble, Cincinnati, USA) under pontic area 12. Similarly, periodontal debridement and restoration of carious teeth were part of the stabilization phase of the treatment.
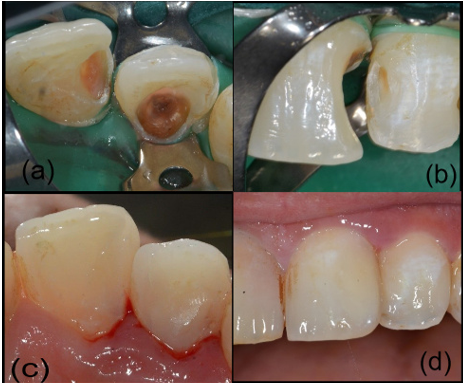
Figure 3 (a-d): Palatal view of cavities preparation in teeth 21 and 22 (a). Labial view of cavities preparation in teeth 21 and 22 (b). Palatal and labial views of completed resin composite restoration in teeth 21 and 22 (c&d)

Figure 4 (a-d): Removal of pontic 12 after two months of healing (a), re-cementation of pontic 12 using SUPER-SPLINT (a&b). Postoperative view after three months of treatment (c). Postoperative view after 10 months of treatment (d).
The purpose of the case report was to illustrate a quick and straightforward chairside technique to replace a single missing tooth in the esthetic zone. There are various such techniques described previously in the literature, but they appear to be cumbersome, time-consuming, and may require laboratory support.6 The current method utilized conventional resin composite readily available in dental clinics to fabricate a pontic. Pontics made of resin composite enable good bond strength with the abutment as similar material is employed for bonding.11 It circumvents the need for grooves and wires required for additional retention when an acrylic denture tooth is used. The tooth mold used is also conveniently available with many resin composite suppliers such as Essentia (GC), Estelite Asteria (Tokuyama Dental, Italy), etc. If tooth mold is not available, the clinician can resort to fabrication of silicone putty matrix using the impression of the tooth on the contralateral side.10
The technique may be utilized as a short-term treatment modality in many clinical scenarios such as provisionalization during a staged implant procedure, tooth loss due to traumatic dental injury, orthodontic space maintenance, and immediate replacement of tooth indicated for extraction. The ovate pontic fitted at the time of tooth extraction has the advantage of papilla preservation, avoidance of black triangles, creating a natural emergence profile, and preventing the need for site development for the bridge.12 In cases where immediate replacement was not planned before the extraction, the site development using gingivoplasty or long-term provisionalization with ovate pontic is advocated to develop the natural emergence profile of the pontic.12 The success of the ovate pontic design depends on how well the patient maintains his oral hygiene. Therefore, the pontic was highly polished as it was critical for cleaning with floss and preventing mucosal inflammation. The patient was reviewed frequently during the treatment phase after the initial cementation of pontic. No complications were noted except for 1-2 mm recession of labial soft tissues. After almost two months of review following completion of root canal treatment of tooth 11, the pontic was removed, its tissue surface adjusted, and it was rebonded with fiber reinforcement as long-term provisional restoration on the patient’s request. The patient was reviewed after 3 and 10 months. He had well-maintained oral hygiene, and no complications were noted.
The imminent loss of an anterior tooth could be a disturbing experience for a patient. Dental practitioners are often challenged with proposing and then assisting the patient in choosing the best course of treatment for their dental problem. The immediate removable partial denture with a socket fit design could have been a choice in this case. However, considering the poor oral hygiene status of the patient and the risk of increased plaque formation, this option was not contemplated. A removable acrylic partial denture requires attention to detail and if not designed and constructed carefully, undesirable stress distribution may lead to detrimental effects.13
The established high success rate of an immediate implant with provisional restoration has paved the way for successfully providing definitive replacement of a lost single tooth in the esthetic zone.5 At first glance, it may look like an appropriate case for immediate implant placement in the extraction socket. However, various factors prevented or contraindicated immediate implant placement in this case. For instance, the neglected oral hygiene, generalized moderate periodontal disease, and periradicular infection may increase the risk of immediate implant failure.14 Furthermore, the treatment options must consider the desires of the patient and their financial capacity. The patient requested to have a minimally invasive and cost-effective replacement option for his broken anterior tooth. Hence, a single-visit chairside technique, which was least invasive and cost-effective as compared to other treatment options, was used.
The variety of clinical scenarios presenting in everyday general dental practice means the clinician has to be prepared with a multitude of immediate tooth replacement techniques for use in the esthetic zone. No one method fits all patients as the indications and patients’ demands differ. The patients are more likely to accept simple, efficient, least invasive, and less expensive treatment options. The technique described in this report, if performed carefully, can provide reasonable short-term provisionalization of missing single teeth in the esthetic zone.