
Total Articles: 43
Today's Visitors: 40

Journal of the Bahrain Medical Society
Year 2014, Volume 25, Issue 2, Pages 105-107
http://doi.org/10.26715/jbms.25_2_10Amal Redha Hubail,* Jinan Harith Darwish*
*Department of Pediatrics, Salmaniya Medical Complex, Kingdom of Bahrain
Correspondence to: dr.amalhubail@gmail.com

The modality of inheritance in CHARGE syndrome is autosomal dominant, classically triggered by mutations in the chromo-domain helicase DNA binding protein-7 (CHD7) gene. CHARGE syndrome is characterized by the variable occurrence of coloboma, heart defects, atresia of the choanae, retarded growth and development, genital hypoplasia, ear anomalies and deafness. In this report, we describe an infant with a typical phenotype characterized by severe psychomotor retardation, facial asymmetry, coloboma, cortical blindness, unilateral choanal atresia, congenital heart anomalies, genital hypoplasia, cranial nerve IX/X dysfunction and global developmental delay that was diagnosed clinically.
Following clinical diagnosis a complete sequencing of the CHD7 gene was carried out at the Institute for Medical Diagnostics GmbH in Ingelheim, Germany. Genomic DNA was screened for mutations in the CD7 gene (OMMIM 608892) on chromosome 8q12.1 The codon exon 2-38 and the respective exon-intron boundaries were amplified by polymerase chain reaction and analysed by direct sequencing. Resulting sequence data were compared with the reference sequence NM_017880.3 No mutation in CHD7 gene was detected as a genetic cause for the clinical phenotype of the patient. The MPLA multiplex ligation-dependent probe amplification analysis showed no copy number variation in the CHD7 gene.
This case report underscores the importance of a detailed family history and physical examination in the diagnosis of CHARGE syndrome. Additionally, it provides valuable insight into the pathogenesis and clinical presentation of the syndrome as well as highlighting the benefits of a multidisciplinary approach. With supportive nurturing care, children with CHARGE syndrome can overcome the associated disabilities and develop necessary motor skills and a life-style enhancing level of fitness.
Keywords: CHARGE syndrome; CHARGE association; Hall-Hittner syndrome; CHD7 gene; empty sella
The acronym CHARGE is used to designate the physical and health issues that are concomitant with the syndrome. CHARGE is a phenotypically heterogeneous syndrome which has been defined as a bundling of clinical features including Coloboma, Heart malformation, Atresia of choanae, Retardation of growth and development, Genital hypoplasia, and Ear anomalies or deafness1. In addition, temporal bone and olfactory nerve anomalies are now considered extremely sensitive for a diagnosis of CHARGE syndrome2.
CHARGE syndrome’s modality of inheritance is autosomal dominant, classically triggered by mutations in the CHD7 gene in roughly two thirds of cases reported3. CHD7 descends from a large family of evolutionarily conserved proteins that are alleged to play a part in chromatin organization. CHD7 is a regulatory element that potentially affects a large sum of developmental pathways, explaining the pleiotropic nature of its phenotypic continuum.
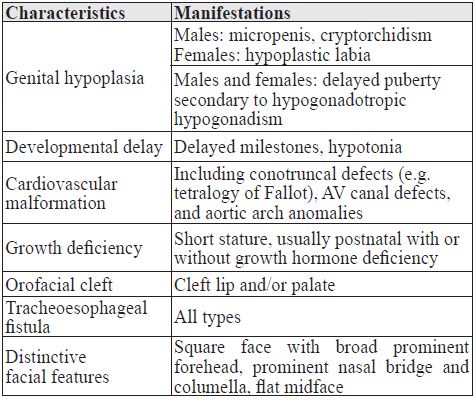
A clinical diagnosis of CHARGE syndrome necessitates the presence of four or more major features or three major features plus three or more minor features4. As a consequence, persons with CHARGE syndrome often require multiple and protracted hospitalizations which in turn can cause developmental delays because of the lack of socialization and physical activity during hospitalizations. See Tables 1 & 2 Post-neonatal death is not a rare event in patients with CHARGE syndrome and it often occurs unexpectedly. Gastro-oesophageal reflux and poor coordination of swallowing and breathing due to cranial nerve dysfunction seem to be the major risk factors5.
Table 1. Major diagnostic characteristics of CHARGE syndrome
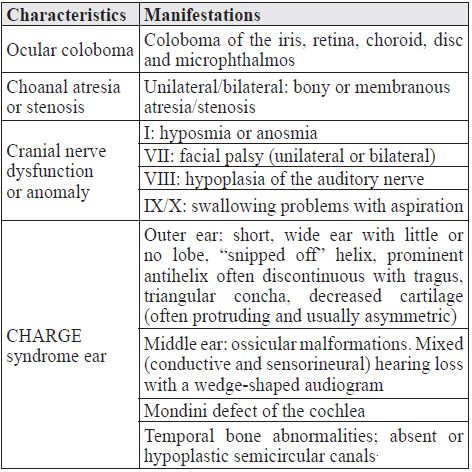
Table 2. Minor diagnostic characteristics of CHARGE syndrome
A Bahraini male IUGR infant aged 18 months, the 1st pregnancy to non-consanguineous phenotypically normal parents. The mother was 19 and the father was 30 years of age at the time of birth of the child.
The mother’s 1st and 2nd trimester histories showed that she had anemia and calcium deficiency for which she was on supplemental iron and calcium. She was also being treated for hypothyroidism. Ultrasound identified oligohydramnios and bilateral dilated ventricles and features of an echogenic bowel. The pregnancy was completed at 36 weeks by induced vaginal delivery for IUGR. Apgar scores were 91 and 95 with a birth weight of 1.65 kg. The neonate was admitted immediately to the NICU with transient tachypnoea of the newborn (TTN) and required mechanical ventilation for two days. His low birth weight necessitated a further twelve week NICU admission.
The pedigree study revealed that the mother had no previous unviable pregnancies and both parents were in good health. One first degree relative was found to have trisomy 21. The window to establishing the diagnosis was the coloboma and dysmorphism noted for the first time by the admitting paediatric resident at the age of 17 weeks. He was tracheostomised and placed on home oxygen at the age of six months due to swallowing problems and in order to avoid accumulation of copious secretion that may obstruct the upper airway. He is currently on home pump nasogastric tube feeding. The mother was instructed by the speech and language therapist on how to do oral stimulation to maintain the infants sucking reflex.
The four major diagnostic characteristics of CHARGE manifested in this specific patient were:
The five minor diagnostic characteristics of CHARGE manifested in this specific patient were:
Vision and fine motor: fixes but does not follow. He is unable to reach out for toys, does not transfer, does not have pincer grasp.
Hearing, speech and language: startles to loud noises. Does not respond to calls but responds to sound. He does not turn to soft sounds and does not vocalize alone or say mama and dada. A tympanogram showed mild asymmetry of hearing loss bilaterally.
Social, emotional and behavioural development: He smiles socially, but does not put food in the mouth, does not wave bye-bye or play peek-a-boo. His need for multiple and prolonged hospitalizations and lack of active management of the sensory deficit have contributed to his developmental delay.
Additional examination:
Additional tests:
The molecular genetic test for diagnosing CHARGE syndrome is a test designed to identify a certain gene which can lead to the diagnosis of this syndrome. This test is however subject to limitations such as being expensive, the complete sequencing of the CHD7 gene costs €2000.00 and the MPLA deletion/duplication analysis of the CHD7 gene costs €500.00. Another limitation of this test is that it is sensitive but not specific as it fails to detect all cases of this syndrome, as is the case with this patient. Mutations in the CHD7 gene are detected in 65-70% of the cases. Rare mutations in the other parts of the gene than those investigated here (e.g. in regulatory regions, low grade mosiacism, larger heterozygous deletions or duplications or mutations in the other genes cannot be excluded with the molecular genetics analysis applied here. Hence, the diagnosis of CHARGE syndrome still remains rather clinical - grounded on the medical features appreciated in the child. The clinical diagnosis is reached using an amalgamation of major and minor features. Major features are features that are fairly collective in CHARGE syndrome but comparatively rare in other conditions, and mostly diagnosable in the neonatal period. Some minor characteristics and features of CHARGE syndrome are not specific to it and thus not clinically useful in distinguishing it from other syndromes.
Management of CHARGE syndrome starts from the first minute of life with providing a secure airway, stabilizing the patient, excluding major life-threatening congenital anomalies. After the initial neonatal and infantile period, individuals with CHARGE syndrome who survive require vigorous restoration of the sensory function to facilitate adequate psychomotor development. Therefore a patient with CHARGE syndrome necessitates a multidisciplinary team approach to deal with different medical issues that arise from this complex syndrome.
It is important to highlight the implications that our greater understanding of the prognosis of CHARGE has for clinical practice and health resource allocation. To this end, it is imperative for clinicians to thoroughly follow up patients in order to tailor therapeutic approaches to their early prognostic indicators and to recognize the development of any comorbid conditions. Ultimately, this may pave the way for improved clinical care of patients with CHARGE. Future research sho uld focus on genetic counseling and modalities to improve the quality of life of these individuals and their families.
In the right environment, patients with CHARGE syndrome have the prospect of developing essential motor skills and a health-enhancing level of fitness. Improvement in their physical activity and education is limited mainly due to the natural history of the syndrome, in addition to the lack of trained specialist to work with the patient and their families.
This report underscores the importance of a detailed family history and physical examination along with the role serendipity and sound clinical judgment played in the diagnosis of CHARGE syndrome in this infant. Good insight about the pathogenesis and the clinical presentation can improve the effectiveness of medical therapies. Further research about CHARGE syndrome is essential in the Gulf Cooperation Council region; particularly the epidemiology, diagnosis and the impact on the quality of life. Additionally, the availability and effectiveness of a multidisciplinary approach to these patients should be studied in order to provide definite evidence for implementation in clinical practice. Finally, we are most certainly in need of a nonprofit, charitable organization in the Kingdom of Bahrain that caters to providing support and educational information to families of children with rare diseases. Hence, becoming instrumental in bringing together parents and professionals involved in their care.